The case: Patient came in for laparoscopic colectomy. She had a history of severe COPD, newly diagnosed adenocarcinoma of colon, anemia (Hb 9), newly diagnosed ANCA vasculitis, h/o mitral stenosis s/p robotic mitral valve replacement, pulmonary HTN, severe TR, systemic HTN, normal EF. Patient had recent exacerbations of CHF with BNP in 1200s. Recent (within the last 3 months) history of coding on induction requiring chest compressions during robotic MVR (50mg propofol). On a steroid taper.
BPs 180-200s/90-110s; PAPs 40-60s/20-40s. 50kg.
Plan: aline, swan, R2, slow induction
Induction: fentanyl 50mcg, propofol 20mg, lidocaine 100mg, etomidate 10mg, roc 50mg. Gtt: epinephrine @ 0.02mcg/kg/min, norepinephrine @ 0.04mcg/kg/min. Milrinone arrived to OR after induction. Able to titrate off epinephrine to Milrinone 0.3mcg/kg/min even with insufflation of abdomen. Did not need to decrease insufflation pressures as hemodynamics were relatively stable.
Extubated safely at the end of the case. Received 100mcg fentanyl, 20mg ketamine, Exparel TAP block, pre-op PO Tylenol 1000mg for pain control. She’s doing well and pleased with her anesthetic management.
Patients with ACS will usually be critically ill and unable to provide history and symptoms. On physical exam, patients present with a distended abdomen. However, palpation and abdominal circumference are not reliable for the diagnosis of ACS[25].
A prospective study in postoperative ICU patients showed physicians have less than a 50% chance to identify IAH by clinical examination[25]. The clinical abdominal exam as IAP assessment has an estimated sensitivity of 56%-60% and specificity of 80%-87%[25,26].
Signs of ACS will present as the end-organ effect from the physiologic changes (Table (Table2).2). The most notorious signs are usually abdominal distention, oliguria, high ventilatory pressures, diminished cardiac output, and metabolic acidosis[26].
The more commonly used method is an indirect measurement such as intravesicular catheter pressures (e.g., Foley catheter), which has become the gold standard due to its widespread availability and limited invasiveness. The trans-bladder technique involves using aseptic clamping the drainage tubing of the Foley then connecting the Foley to a three-way stop tap adjusted to the level of the mid-axillary line at the iliac crest to zero transducers follow by injecting 25 cc of sterile saline into the bladder. Measurements should be taken at end-expiration and complete supine position and expressed in mmHg. Bladder pressures below 5 mm Hg are expected in healthy patients. Pressures between 10 to 15 mm Hg can be expected following abdominal surgery and in obese patients. Bladder pressures over 25 mm Hg are highly suspicious of abdominal compartment syndrome and should be correlated clinically. It is recommended that pressure measurements be trended to show and recognize the worsening of intra-abdominal hypertension.
Contraindications to using bladder pressures include bladder trauma, neurogenic bladder, BPH, and pelvic hematoma. Bladder pressures may be inaccurate if the patient is not sedated or lying flat.[9][10]
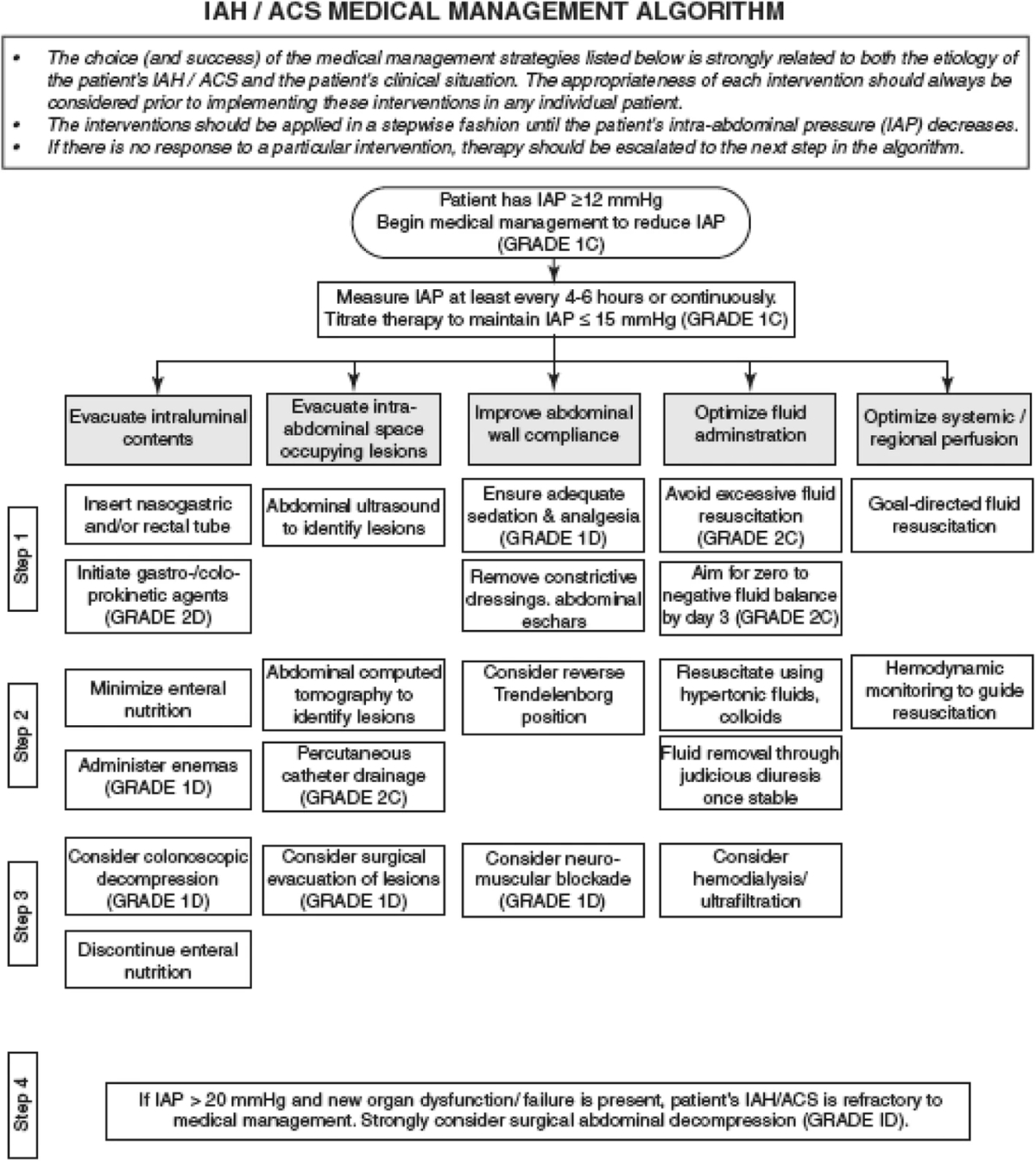
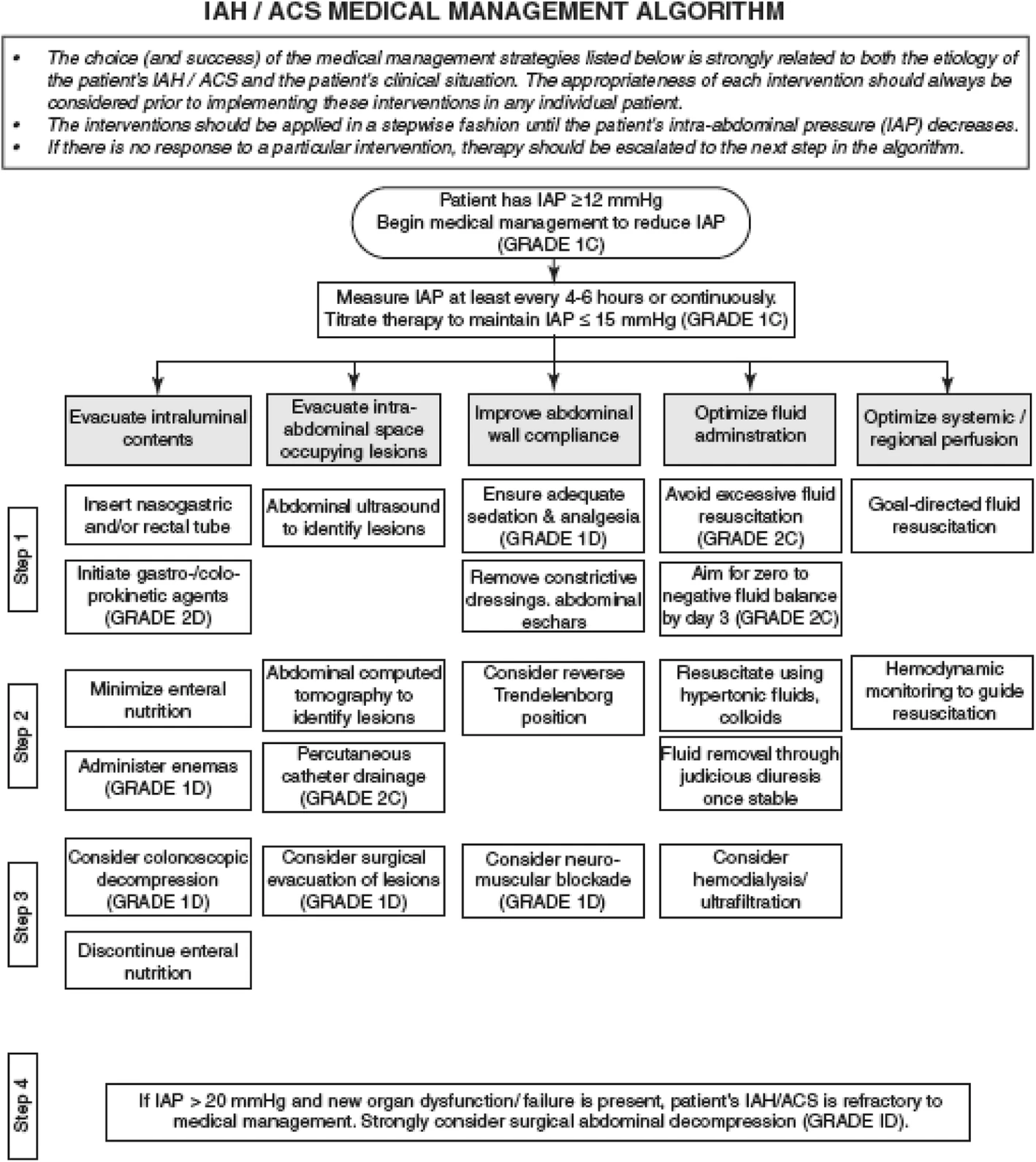
The primary treatment for ACS is surgical decompression. However, the early use of non-surgical interventions may prevent the progression of IAH to ACS. Early recognition involves supportive care to include keeping patients comfortable with pain well-controlled. Decompressive procedures such as NG tube placement for gastric decompression, rectal tube placement for colonic decompression, and percutaneous drainage of abscesses, ascites, or fluid from the abdominal compartment. The neuromuscular blockade has been described to be used as a brief trial in an attempt to relax the abdominal musculature, leading to a significant decrease in abdominal compartment pressures in the ventilated ICU patient. If conservative and medical management does not resolve the IAH and further organ damage is noted, surgical decompression using emergent laparotomy may be considered. [11][2]
After surgical laparotomy for compartment syndrome, the abdominal fascia may be closed using temporary closure devices such as (vacs, meshes, and zippers). The fascia can be appropriately closed after 5 to 7 days after the compartment pressures and swelling have decreased.