Medicare’s geographic adjustment for a particular physician payment locality is determined using three geographic practice cost indices (GPCI) that correspond to the three components of a Medicare fee–physician work, practice expense, and malpractice expense.
Physician work–the financial value of physicians’ time, skill, and effort that are associated with providing the service.
Practice expense–the costs incurred by physicians in employing office staff, renting office space, and buying supplies and equipment.
Malpractice expense–the premiums paid by physicians for professional liability insurance. Each RVU measures the relative costliness of providing a particular service.
These GPCIs adjust physician fees for variations in physicians’ costs of providing care in different payment localities. Specifically, they raise or lower Medicare fees depending on whether a payment locality’s average cost of operating a physician practice is above or below the national average. CMS is required to review the GPCIs at least every 3 years and, at that time, may update them using more recent data. The major data source used in calculating the GPCIs, the decennial census, provides new data once every 10 years. The GPCIs were last updated in 2005 and CMS is scheduled to review and, if necessary, update them again in 2008. Concerns have been raised in Congress and among stakeholders, including state medical associations, that the geographic boundaries of some payment localities do not accurately address variations in the costs of operating a private medical practice. If they do not, beneficiaries could potentially experience problems accessing physician services.
More than half of the current physician payment localities had at least one county within them with a large payment difference–that is, there was a payment difference of 5 percent or more between physicians’ costs and Medicare’s geographic adjustment for an area. Overall, there were 447 counties with large payment differences–representing 14 percent of all counties. These counties were located across the United States, but a disproportionate number were located in five states. Specifically, 60 percent of counties with large payment differences were located in California, Georgia, Minnesota, Ohio, and Virginia. Large payment differences occur because many payment localities combine counties with very different costs, which may be attributed to several factors. For example, although substantial population growth has occurred in certain geographic areas, potentially leading to increased costs, CMS has not revised the payment localities to reflect these changes.
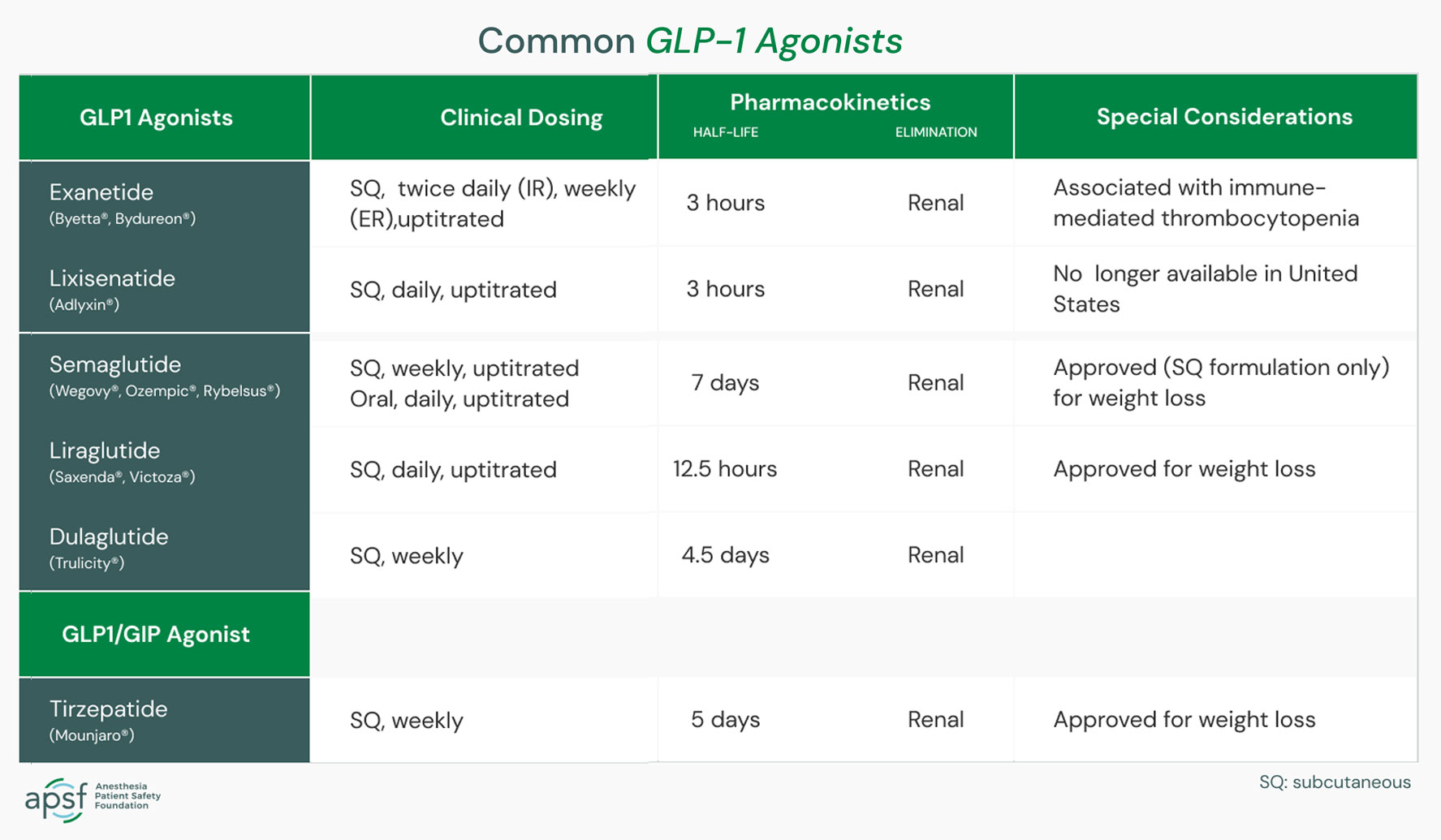
ASA’s Task Force on Preoperative Fasting suggests the following for patients taking GLP-1 agonists for type 2 diabetes or weight loss who are having elective procedures. It is also calling for further research to be done regarding GLP-1 agonist medications and anesthesia.
Day or week prior to the procedure:
Hold GLP-1 agonists on the day of the procedure/surgery for patients who take the medication daily.
Hold GLP-1 agonists a week prior to the procedure/surgery for patients who take the medication weekly.
Consider consulting with an endocrinologist for guidance in patients who are taking GLP-1 agonists for diabetes management to help control their condition and prevent hyperglycemia (high blood sugar).
Day of the procedure:
Consider delaying the procedure if the patient is experiencing GI symptoms such as severe nausea/vomiting/retching, abdominal bloating or abdominal pain and discuss the concerns of potential risk of regurgitation and aspiration with the proceduralist or surgeon and the patient.
Continue with the procedure if the patient has no GI symptoms and the GLP-1 agonist medications have been held as advised.
If the patient has no GI symptoms, but the GLP-1 agonist medications were not held, use precautions based on the assumption the patient has a “full stomach” or consider using ultrasound to evaluate the stomach contents. If the stomach is empty, proceed as usual. If the stomach is full or if the gastric ultrasound is inconclusive or not possible, consider delaying the procedure or proceed using full stomach precautions. Discuss the potential risk of regurgitation and aspiration of gastric contents with the proceduralist or surgeon and the patient.
Full stomach precautions also should be used in patients who need urgent or emergency surgery.
It seems that ever since that advent of dexmedetomidine, propofol has been pushed aside as the sedation drug of choice for sedation during and post-open heart surgery. But is the literature changing with the effects of dexmedetomidine on rates of atrial fibrillation?
In patients older than 60 years with low baseline risk of postoperative delirium admitted to the ICU after cardiac surgery and extubated within 12 h of ICU admission, a post-extubation nighttime dose of dexmedetomidine may reduce the incidence of delirium on postoperative day one.
The study results showed no statistically significant difference between both groups with regard to age and body mass index. Group P patients were more associated with lower MAP and HR than Group D patients. There was no statistically significant difference between groups with regard to ABG findings, oxygenation, ventilation, and respiratory parameters. There was significant difference between both the groups in midazolam and fentanyl dose requirement and financial costs with a value of P < 0.05.
Meta-analysis studies on the use of DEX during cardiac surgery also showed a reduction in the risk of atrial fibrillation, ventricular tachycardia and cardiac arrest [7, 12].
Our findings suggest that DEX may reduce short term postoperative pulmonary complications, time on mechanical lung ventilation, ICU and hospital stay following CABG surgery compared to propofol.
When compared with propofol, dexmedetomidine sedation reduced incidence, delayed onset, and shortened duration of POD in elderly patients after cardiac surgery. The absolute risk reduction for POD was 14%, with a number needed to treat of 7.1.
Dexmedetomidine did not significantly impact ICU length of stay compared with propofol, but it significantly reduced the duration of mechanical ventilation and the risk of delirium in cardiac surgical patients. It also significantly increased the risk of bradycardia across ICU patient subsets.
The use of dexmedetomidine for sedation after cardiac surgery was associated with a lower incidence of atrial fibrillation and hence decreased the duration of intensive care stay.
This trial demonstrated that dexmedetomidine sedation may be better able to improve microcirculation in cardiac surgery patients during the early postoperative period compared with propofol.
Adding low-dose rate dexmedetomidine to a sedative regimen based on propofol did not result in a different risk of in-hospital delirium in older patients undergoing cardiac surgery. With a suggestion of both harm and benefit in secondary outcomes, supplementing postoperative propofol with dexmedetomidine cannot be recommended based on this study.
Dexmedetomidine infusion, started at anaesthetic induction and continued for 24 h, did not decrease postoperative atrial arrhythmias in patients recovering from cardiac surgery. Dexmedetomidine also worsened delirium, although not by a significant amount, possibly by provoking hypotension. Dexmedetomidine worsened kidney injury, but again not by a significant amount. The incidence of persistent surgical pain was similar in each group. Dexmedetomidine should be used cautiously in cardiac surgical patients with attention to preventing hypotension, and should not be given in expectation of reducing atrial fibrillation or delirium.
Dexmedetomidine-based sedation resulted in achievement of early extubation more frequently than propofol- based sedation. Mean postoperative time to extubation and average hospital LOS were shorter with dexmedetomidine- based sedation and met a statistical level of significance. There was no difference in ICU-LOS or in-hospital mortality between the two groups. Total hospital charges were similar, although slightly higher in the propofol group.
One means of achieving a balanced resuscitation is with the use of WB instead of component therapy. The combination of plasma, PLT and PRBC components in a 1:1:1 ratio is estimated to result in a HCT of 25%, coagulation factor activity of 62%, platelet concentration of 50×109/L, and fibrinogen concentration of 75 mg/dL. In comparison, a unit of fresh WB has a HCT of 45%, 100% activity of all coagulation factors, platelet concentration of 200×109/L, and fibrinogen concentration of 150 mg/dL
The American College of Obstetricians and Gynecologists (ACOG) recommends fixed product ratios (65). This practice is supported by retrospective studies that demonstrate, in combination with a comprehensive post-partum hemorrhage protocol, MTP is associated with improvement in transfusion needs and peri-partum hysterectomy (66–68). Additionally, obstetric hemorrhage protocols should focus on repletion of fibrinogen via early administration of CRYO or fibrinogen concentrate, as fibrinogen is the first coagulation factor to diminish in post-partum hemorrhage
In addition to blood transfusion during MTP, several useful pharmacologic adjuncts to resuscitation have been identified. These include calcium repletion, tranexamic acid (TXA), factor VII concentrate, prothrombin complex concentrate (PCC), and arginine vasopressin (AVP). In addition to pharmacologic adjuncts, the use of viscoelastic testing can help improve blood product utilization and outcomes.
One in 455 blood components transfused is associated with an adverse event, but the risk of serious adverse reactions (1 in 6,224) and transfusion-transmitted infections (1 in 255,400) is extremely low in the United States (117). The most common non-infectious reactions include febrile non-hemolytic transfusion reactions, allergic transfusion reactions, transfusion-associated circulatory overload (TACO), transfusion-related acute lung injury (TRALI), and acute or delayed hemolytic reactions (118). The effects of blood preservation and storage also cause changes in the quality of the blood over time, including decreased pH, increased potassium, decreased 2,3-diphosphoglycerate (2,3-DPG), and decreases in erythrocyte and platelet function, all of which may affect resuscitation and oxygen delivery (119).
Trigger for FFP and/or PCC in Clinical Recommendations
In the Society of Cardiac Anesthesiology recommendations, transfusion of 10 to 15 ml/kg of FFP or a low dose of PCC (not defined) is recommended when clotting time in tissue factor–activated ROTEM or the reaction time in heparinase TEG is significantly prolonged (table 2).13 Of note, the European recommendations for hemostatic resuscitation in trauma recommend a dose of 25 IU/kg of a PCC, whereas in cardiac surgery patients, an initial dose of 12.5 IU/kg (similar to that suggested by the U.S. recommendations) should be considered because of the inherent risk of thromboembolism.20 In the European trauma guidelines, the authors point out the possible influence of hypofibrinogenemia on clotting time in tissue factor–activated ROTEM.14 Therefore, PCC should be given only when fibrinogen levels are less than 1.5 g/l (corresponding to a fibrinogen ROTEM maximal clot firmness of less than 10 mm), and clotting time in tissue factor–activated ROTEM is prolonged or remains prolonged after replacement of fibrinogen.
− SWB, which will in U.S. military practice be LTOWB, is the preferred product for resuscitation of severe bleeding (both pre-hospital and in-hospital). SWB simplifies the logistics of the transfusion and may facilitate more rapid resuscitation of casualties, and may enhance a facility’s capacity to manage mass casualty (MASCAL) challenges.
− The indication for SWB is life-threatening hemorrhage. The assessment that a hemorrhage is life-threatening is mainly established clinically, and should be driven by an assessment of the patient’s vital signs, hemodynamics, physical exam, mechanism of injury and laboratory measures of shock and hemostasis if available. The use of FWB should be reserved for when SWB or full component therapy is unavailable.
− Blood component therapy (1:1:1) is an acceptable option for treating life-threatening hemorrhage when SWB is not available. The potential reduced efficacy, safety, and logistical aspects of blood component therapy should be taken into consideration when choosing between resuscitation strategies (Table I).
In the massively bleeding patient with coagulopathy, our group recommends the administration of an initial bolus of 25 IU.kg-1. This applies for: the acute reversal of vitamin K antagonist therapy; haemostatic resuscitation, particularly in trauma; and the reversal of direct oral anticoagulants when no specific antidote is available.
In patients with a high risk for thromboembolic complications, e.g. cardiac surgery, the administration of an initial half-dose bolus (12.5 IU.kg-1) should be considered.
A second bolus may be indicated if coagulopathy and microvascular bleeding persists and other reasons for bleeding are largely ruled out. Tissue-factor-activated, factor VII-dependent and heparin insensitive point-of-care tests may be used for peri-operative monitoring and guiding of prothrombin complex concentrate therapy.
For the endpoint of rapid INR reduction, the results from our trial are consistent with previously published (mainly observational) data and demonstrate that 4F-PCC is non-inferior and superior to plasma for rapid INR reduction in patients on VKA therapy.
Furthermore, we noted that 4F-PCC could be given more rapidly than plasma, which is in agreement with previously published (retrospectively collected) data.24
For the endpoint of clinical efficacy, we found no other adequately powered trial examining reversal of VKA therapy in patients needing urgent surgical procedures, and this trial therefore offers new insights into their treatment. We noted that 4F-PCC was superior to plasma for haemostatic efficacy.
Although our study was not powered to assess safety, we did not detect any between-treatment differences for the occurrence of thromboembolic events or deaths, a finding in agreement with the existing scientific literature.11, 17, 25, 26 Additionally, although these data guide clinicians on how best to achieve urgent VKA reversal, the scientific literature concerning which patients should be urgently reversed before surgical or invasive interventions continues to evolve; for example, findings from a recent trial showed the safety of pacemaker placement without interruption of anticoagulation.29
Among the key recommendations in this article are the following:
For dosing of VKAs, we recommend the initiation of oral anticoagulation therapy, with doses between 5 mg and 10 mg for the first 1 or 2 days for most individuals, with subsequent dosing based on the international normalized ratio (INR) response (Grade 1B); we suggest against pharmacogenetic-based dosing until randomized data indicate that it is beneficial (Grade 2C); and in elderly and other patient subgroups who are debilitated or malnourished, we recommend a starting dose of ≤ 5 mg (Grade 1C). The article also includes several specific recommendations for the management of patients with nontherapeutic INRs, with INRs above the therapeutic range, and with bleeding whether the INR is therapeutic or elevated.
For the use of vitamin K to reverse a mildly elevated INR, we recommend oral rather than subcutaneous administration (Grade 1A).
For most patients who have a lupus inhibitor, we recommend a therapeutic target INR of 2.5 (range, 2.0 to 3.0) [Grade 1A].
We recommend that physicians who manage oral anticoagulation therapy do so in a systematic and coordinated fashion, incorporating patient education, systematic INR testing, tracking, follow-up, and good patient communication of results and dose adjustments [Grade 1B].
In patients who are suitably selected and trained, patient self-testing or patient self-management of dosing are effective alternative treatment models that result in improved quality of anticoagulation management, with greater time in the therapeutic range and fewer adverse events. Patient self-monitoring or self-management, however, is a choice made by patients and physicians that depends on many factors. We suggest that such therapeutic management be implemented where suitable (Grade 2B).
In patients on VKA therapy presenting with severe hemorrhage, international guidelines recommend, as soon as the diagnosis is confirmed, the administration of PCC (≥20 UI/kg) and vitamin K (≥5 mg) to normalize coagulation (post-reversal INR ≤1.5).
A guideline-concordant administration dose of PCC and vitamin K administrated in the first eight hours was associated with a two-fold decrease in seven-day mortality overall and with a three-fold decrease in the ICH subgroup
The guideline-concordant reversal was performed in 38% of the patients within eight hours after admission
Whereas pre-reversal INR is not absolutely necessary, post-reversal INR is essential to evaluate treatment efficacy
The post-reversal INR target must be performed systematically and immediately after PCC administration
The case: Patient came in for laparoscopic colectomy. She had a history of severe COPD, newly diagnosed adenocarcinoma of colon, anemia (Hb 9), newly diagnosed ANCA vasculitis, h/o mitral stenosis s/p robotic mitral valve replacement, pulmonary HTN, severe TR, systemic HTN, normal EF. Patient had recent exacerbations of CHF with BNP in 1200s. Recent (within the last 3 months) history of coding on induction requiring chest compressions during robotic MVR (50mg propofol). On a steroid taper.
BPs 180-200s/90-110s; PAPs 40-60s/20-40s. 50kg.
Plan: aline, swan, R2, slow induction
Induction: fentanyl 50mcg, propofol 20mg, lidocaine 100mg, etomidate 10mg, roc 50mg. Gtt: epinephrine @ 0.02mcg/kg/min, norepinephrine @ 0.04mcg/kg/min. Milrinone arrived to OR after induction. Able to titrate off epinephrine to Milrinone 0.3mcg/kg/min even with insufflation of abdomen. Did not need to decrease insufflation pressures as hemodynamics were relatively stable.
Extubated safely at the end of the case. Received 100mcg fentanyl, 20mg ketamine, Exparel TAP block, pre-op PO Tylenol 1000mg for pain control. She’s doing well and pleased with her anesthetic management.