It seems that ever since that advent of dexmedetomidine, propofol has been pushed aside as the sedation drug of choice for sedation during and post-open heart surgery. But is the literature changing with the effects of dexmedetomidine on rates of atrial fibrillation?
In patients older than 60 years with low baseline risk of postoperative delirium admitted to the ICU after cardiac surgery and extubated within 12 h of ICU admission, a post-extubation nighttime dose of dexmedetomidine may reduce the incidence of delirium on postoperative day one.
The study results showed no statistically significant difference between both groups with regard to age and body mass index. Group P patients were more associated with lower MAP and HR than Group D patients. There was no statistically significant difference between groups with regard to ABG findings, oxygenation, ventilation, and respiratory parameters. There was significant difference between both the groups in midazolam and fentanyl dose requirement and financial costs with a value of P < 0.05.
Meta-analysis studies on the use of DEX during cardiac surgery also showed a reduction in the risk of atrial fibrillation, ventricular tachycardia and cardiac arrest [7, 12].
Our findings suggest that DEX may reduce short term postoperative pulmonary complications, time on mechanical lung ventilation, ICU and hospital stay following CABG surgery compared to propofol.
When compared with propofol, dexmedetomidine sedation reduced incidence, delayed onset, and shortened duration of POD in elderly patients after cardiac surgery. The absolute risk reduction for POD was 14%, with a number needed to treat of 7.1.
Dexmedetomidine did not significantly impact ICU length of stay compared with propofol, but it significantly reduced the duration of mechanical ventilation and the risk of delirium in cardiac surgical patients. It also significantly increased the risk of bradycardia across ICU patient subsets.
The use of dexmedetomidine for sedation after cardiac surgery was associated with a lower incidence of atrial fibrillation and hence decreased the duration of intensive care stay.
This trial demonstrated that dexmedetomidine sedation may be better able to improve microcirculation in cardiac surgery patients during the early postoperative period compared with propofol.
Adding low-dose rate dexmedetomidine to a sedative regimen based on propofol did not result in a different risk of in-hospital delirium in older patients undergoing cardiac surgery. With a suggestion of both harm and benefit in secondary outcomes, supplementing postoperative propofol with dexmedetomidine cannot be recommended based on this study.
Dexmedetomidine infusion, started at anaesthetic induction and continued for 24 h, did not decrease postoperative atrial arrhythmias in patients recovering from cardiac surgery. Dexmedetomidine also worsened delirium, although not by a significant amount, possibly by provoking hypotension. Dexmedetomidine worsened kidney injury, but again not by a significant amount. The incidence of persistent surgical pain was similar in each group. Dexmedetomidine should be used cautiously in cardiac surgical patients with attention to preventing hypotension, and should not be given in expectation of reducing atrial fibrillation or delirium.
Dexmedetomidine-based sedation resulted in achievement of early extubation more frequently than propofol- based sedation. Mean postoperative time to extubation and average hospital LOS were shorter with dexmedetomidine- based sedation and met a statistical level of significance. There was no difference in ICU-LOS or in-hospital mortality between the two groups. Total hospital charges were similar, although slightly higher in the propofol group.
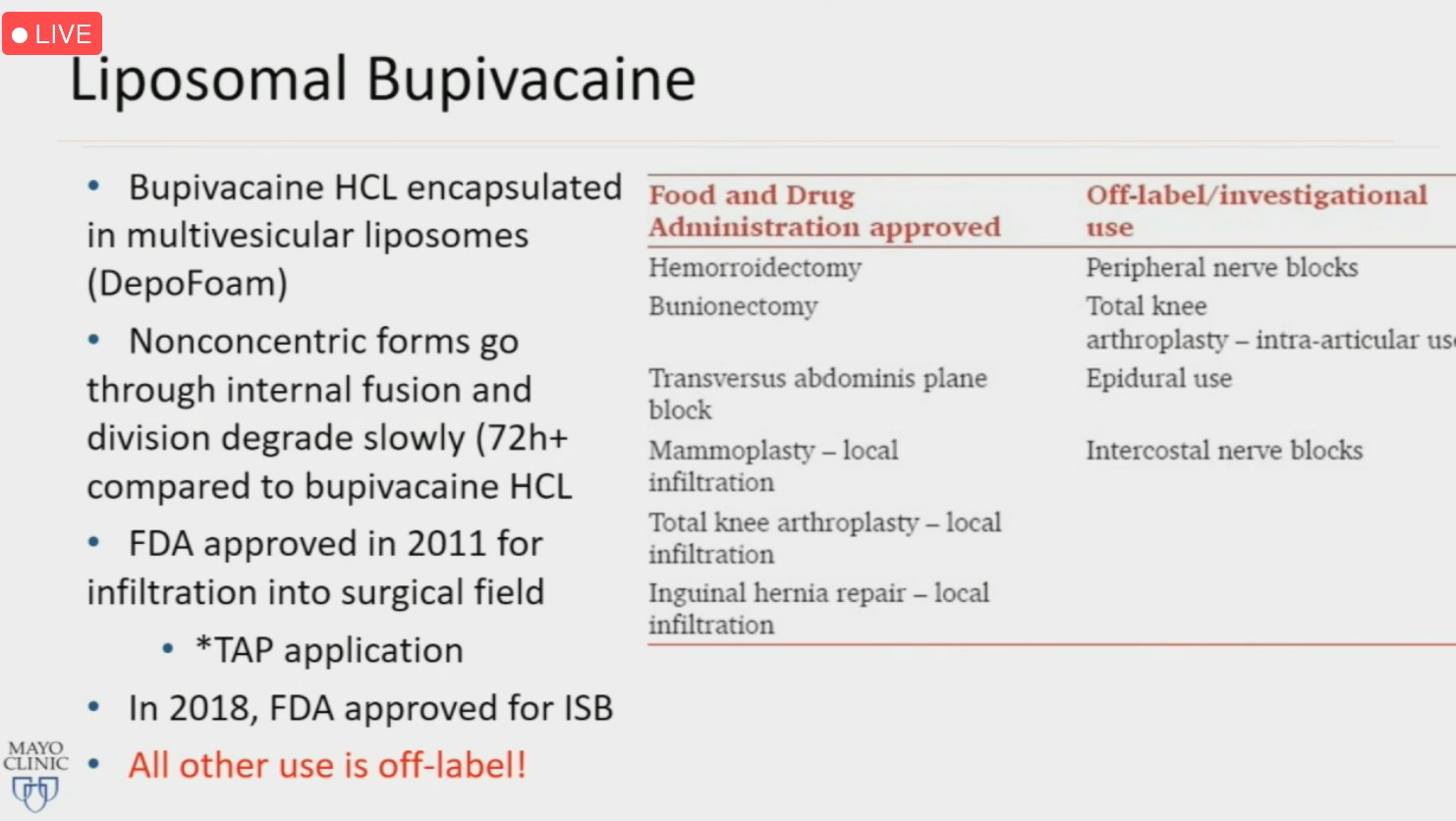
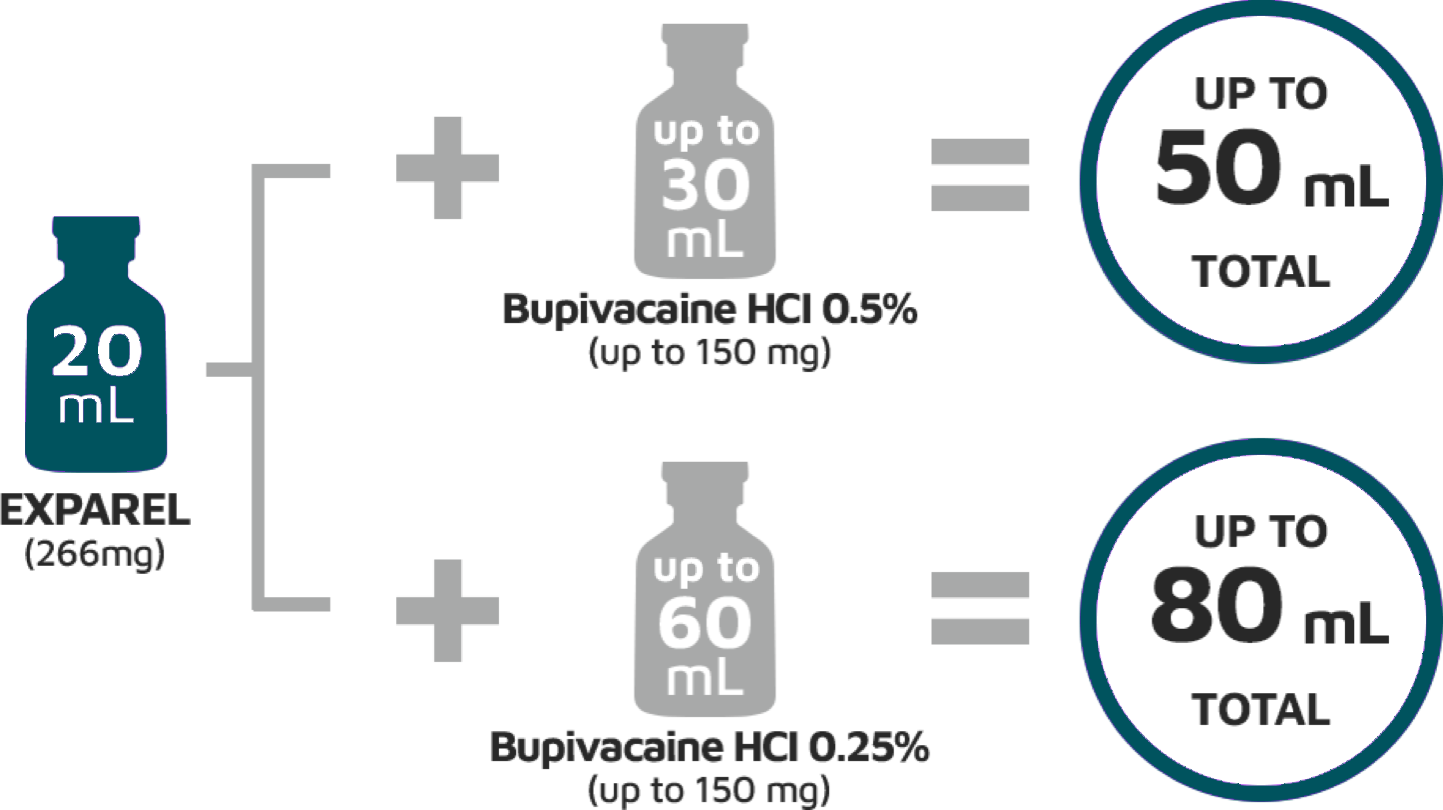
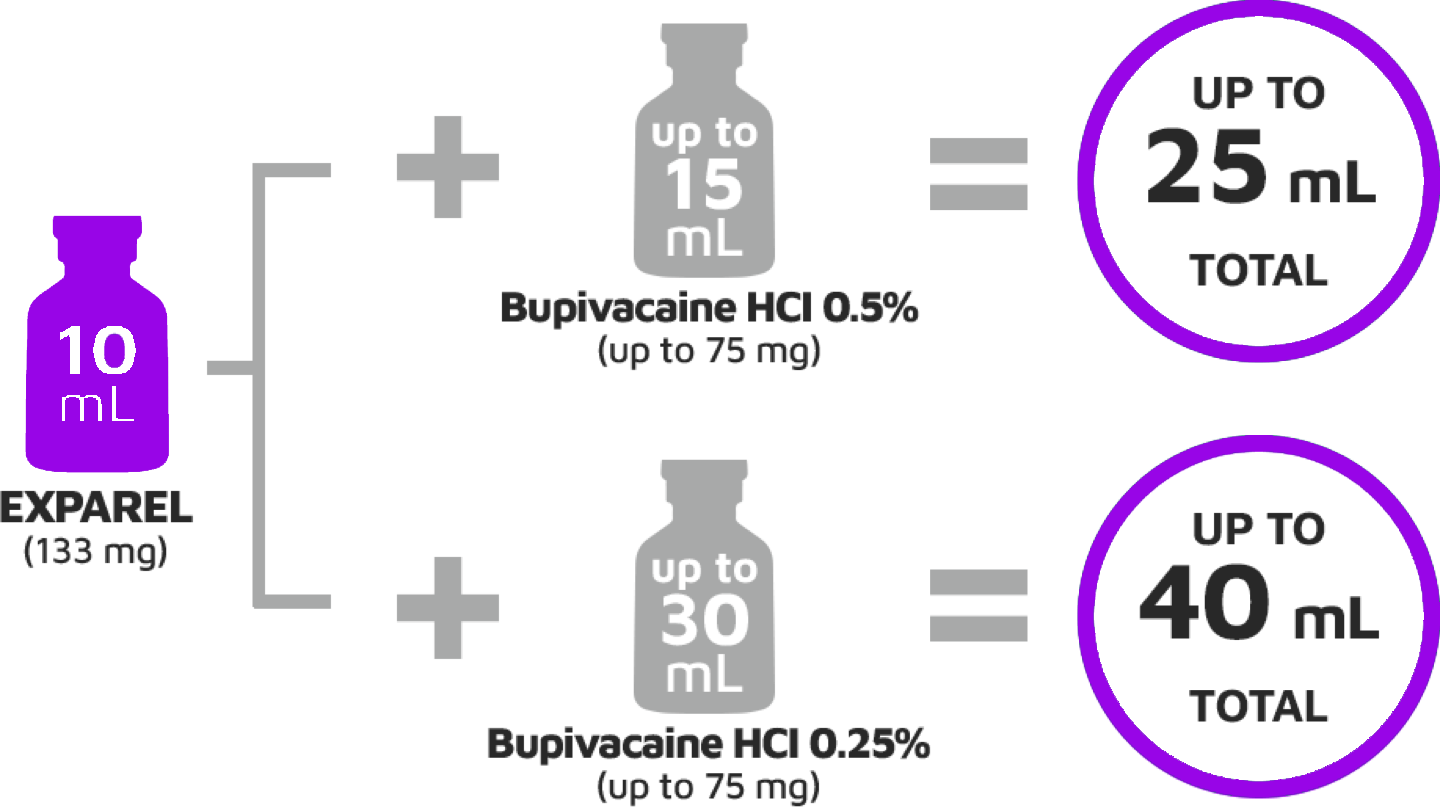
Liposomal bupivacaine (Exparel) is a longer acting form of traditional bupivacaine that delivers the drug by means of a multivesicular liposomal system.
VATs: Dilute liposomal bupivacaine (266 mg, 20 cc) mixed with 20 cc injectable saline. We use two syringes to save time (refill syringe between injections).
For planned thoracotomy, we add 60 cc injectable saline for wider injection.
The efficacy of this strategy requires attention to specific details, such as timing and technique of injection, dilution with saline, and injection of multiple interspaces (typically interspaces 3–10 when technically possible).
Inject EXPAREL slowly and deeply (generally 1-2 mL per injection) into soft tissues using a moving needle technique (ie, inject while withdrawing the needle)
Infiltrate above and below the fascia and into the subcutaneous tissue
Aspirate frequently to minimize the risk of intravascular injection
Use a 25-gauge or larger-bore needle to maintain the structural integrity of the liposomal particles
Inject frequently in small areas (1-1.5 cm apart) to ensure overlapping analgesic coverage
0.2 mg/kg of methadone (based on ideal body weight, up to a maximal dose of 20 mg)250 mg of ketamine was added to the dextrose 5% in water bag (total volume 500 ml). 500 ml bags were connected to a pump that was programed to deliver an infusion of ketamine dosed at ideal body weight (or an equal volume of dextrose 5% in water) at a rate of 0.3 mg · kg−1 · h−1 from induction of anesthesia until surgical closure, at which time the infusion was decreased to 0.1 mg · kg−1 · h−1. The infusion was maintained at a rate of 0.1 mg · kg−1 · h−1 in the postanesthesia care unit (PACU) and for the next 48 postoperative hours. Dosing of ketamine was based on recommendations in the literature17,18 and from clinical experience at our institution.
Patient risk factors (including female gender, non-smoker, history of PONV, or motion sickness) could be quantified using risk scores such as the Apfel score and the Koivuranta score, while surgical procedures such as laparotomy and cholecystectomy confer additional PONV risk. Other perioperative risk factors of PONV includes the length of surgery, the use of volatile anesthesia, including nitrous oxide, as well as perioperative opioid administration. Perioperative risk reduction interventions include multimodal, opioid sparing anesthesia, avoidance of volatile anesthetic, as well as nitrous oxide exposure. Gan et al2 have extensively reviewed various options for PONV prophylaxis and rescue treatment, which includes pharmacological and non-pharmacological interventions. The authors acknowledged that currently the biggest challenge in PONV management is often low compliance to the guidelines.
Fig 1. Summary of the expert consensus guidelines on postoperative nausea and vomiting (PONV) management.
Palonosetron monotherapy for PONV prophylaxis is more effective than other 5-HT3 antagonists, including ondansetron, granisetron, ramosetron; it is also more effective than dexamethasone. Palonosetron has comparable efficacy to aprepitant.
Aprepitant is a competitive Neurokinin (NK)-1 receptor antagonist which was also initially approved for the treatment of chemotherapy-induced nausea and vomiting. It is administered orally, although an intravenous equivalent is also available, in the form of a pro-drug Fosaprepitant. It has a half-life of 9–13 hours, and it has been suggested that its duration of action may be as long as 40 hours. Fosaprepitant is approved only for chemotherapy-induced nausea and vomiting. As a single agent prophylaxis, 40 mg aprepitant has similar efficacy as 0.075 mg palonosetron. Clinical trials and meta-analyses have reported that aprepitant is more effective in preventing PONV when compared to ondansetron. Similar to palonosetron, the aprepitant is also shown to be beneficial in ambulatory surgery due to its long duration of action and lower risk of postdischarge nausea and vomiting. Vallejo et al59 conducted a clinical trial of 150 patients with moderate-to-high risk undergoing ambulatory plastic surgery, and found that aprepitant plus ondansetron was associated with significantly lower incidence of postdischarge nausea and vomiting than ondansetron alone.
Amisulpride is a dopamine receptors antagonist. While initially licensed as an antipsychotic, in February 2020 the FDA approved its IV formulation for prophylactic and rescue therapy of PONV. The anti-emetic dose for prophylaxis is 5 mg IV, 10 mg IV for rescue treatment, whereas its antipsychotic dose is 50–1,200 mg/day orally.
This study found that the antiemetic efficacy of ondansetron and aprepitant was comparable in preventing PONV in patients undergoing thyroidectomy and mastectomy. We found both ondansetron and aprepitant were equally efficacious in preventing emetic episodes, reducing the incidence of nausea and delaying the time to request of a rescue antiemetic. Although not statistically significant, the aprepitant group had a higher incidence of vomiting in the 12-24 h period. However, this group took longer to develop the first episode of vomiting and also to receive the first dose of rescue antiemetic, when compared with ondansetron group. Although the ondansetron group had less vomiting after 12 h, there was a higher incidence of nausea (both being statistically insignificant). So, overall there was no statistically significant difference in the incidence of PONV in both the groups.
BJA:Aug2007, Vol99;Issue2,P202-211. Fig4. Kaplan–Meier curves for the time to first vomiting during the 48 h after surgery.BJA. Fig 3 Proportions of patients with no vomiting 0–24 and 0–48 h after surgery, by treatment group (modified intent-to-treat population). For each group, the error bar represents the value of the upper bound of the 95% CI for the percentage of patients achieving the endpoint. For 0–24 h, n = 293 for aprepitant 40 mg, n = 293 for aprepitant 125 mg, and n = 280 for ondansetron 4 mg. For 0–48 h, n = 292 for aprepitant 40 mg, n = 290 for aprepitant 125 mg, and n = 279 for ondansetron 4 mg.
Results
Aprepitant at both doses was non-inferior to ondansetron for complete response 0–24 h after surgery (64% for aprepitant 40 mg, 63% for aprepitant 125 mg, and 55% for ondansetron, lower bound of 1-sided 95% CI > 0.65), superior to ondansetron for no vomiting 0–24 h after surgery (84% for aprepitant 40 mg, 86% for aprepitant 125 mg, and 71% for ondansetron; P < 0.001), and superior for no vomiting 0–48 h after surgery (82% for aprepitant, 40 mg, 85% for aprepitant, 125 mg, and 66% for ondansetron; P < 0.001). The distribution of peak nausea scores was lower in both aprepitant groups vs ondansetron (P < 0.05).
Conclusions
Aprepitant was non-inferior to ondansetron in achieving complete response for 24 h after surgery. Aprepitant was significantly more effective than ondansetron for preventing vomiting at 24 and 48 h after surgery, and in reducing nausea severity in the first 48 h after surgery. Aprepitant was generally well tolerated.
Fourteen RCTs were included. Meta-analysis found that 80 mg of aprepitant could reduce the incidences of nausea (3 RCTs with 224 patients, pooled risk ratio (RR) = 0.60, 95% confidence interval (CI) = 0.47 to 0.75), and vomiting (3 RCTs with 224 patients, pooled RR = 0.13, 95% CI = 0.04 to 0.37) compared with placebo. Neither 40 mg (3 RCTs with 1171 patients, RR = 0.47, 95% CI = 0.37 to 0.60) nor 125 mg (2 RCTs with 1058 patients, RR = 0.32, 95% CI = 0.13 to 0.78) of aprepitant showed superiority over 4 mg of ondansetron in preventing postoperative vomiting. NMA did not find a dose-dependent effect of aprepitant on preventing postoperative vomiting.
Limited data suggested that NK-1R antagonists, especially aprepitant were effective in preventing PONV compared with placebo. More large-sampled high-quality RCTs are needed.
In conclusion, our study found that NK-1R antagonists, especially aprepitant, helped preventing PONV in patients undergoing surgery with general anesthesia by decreasing the incidence of nausea and vomiting, and delaying the time to first vomiting. However, more data from high-quality RCTs and a comprehensive evaluation of related adverse events were needed before a recommendation of using NK-1R antagonists to prevent PONV could be made.
Postoperative nausea and vomiting (PONV) are common and distressing to patients. The general incidence of vomiting is about 30%, the incidence of nausea is about 50%, and in a subset of high-risk patients, the PONV rate can be as high as 80%. Unresolved PONV may result in prolonged postanesthesia care unit (PACU) stay and unanticipated hospital admission that result in a significant increase in overall health care costs. The goal of PONV prophylaxis is therefore to decrease the incidence of PONV and thus patient-related distress and reduce health care costs.
Figure 1: Risk score for PONV in adults. Simplified risk score from Apfel et al.9 to predict the patient’s risk for PONV. When 0, 1, 2, 3, and 4 of the risk factors are present, the corresponding risk for PONV is about 10%, 20%, 40%, 60%, and 80%, respectively. PONV = postoperative nausea and vomiting.Figure 2 Simplified risk score for PDNV in adults. Simplified risk score from Apfel et al.19 to predict the risk for PDNV in adults. When 0, 1, 2, 3, 4, and 5 risk factors are present, the corresponding risk for PDNV is approximately 10%, 20%, 30%, 50%, 60%, and 80%, respectively. PDNV = postdischarge nausea and vomiting; PONV = postoperative nausea and vomiting; PACU = postanesthesia care unit.Table 2: Strategies to Reduce Baseline Risk. Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesthesia & Analgesia118(1):85-113, January 2014.Table 3. Antiemetic Doses and Timing for Prevention of PONV in Adults. Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesthesia & Analgesia118(1):85-113, January 2014.Figure 4. Algorithm for management of postoperative nausea and vomiting. PONV = postoperative nausea and vomiting. Consensus Guidelines for the Management of Postoperative Nausea and Vomiting Anesthesia & Analgesia118(1):85-113, January 2014.Table 4. Pharmacologic Combination Therapy for Adults and Children. Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesthesia & Analgesia118(1):85-113, January 2014.
Ondansetron is also as effective as dexamethasone and haloperidol 1 mg IV, with no difference in effect on the QTc interval. However, it is less effective than aprepitant for reducing emesis and palonosetron for the incidence of PONV.
Compared with palonosetron 0.075 mg, granisetron 2.5 mg is as effective at 3 hours and 3 to 24 hours but less effective at 24 to 48 hours. Palonosetron 0.075 mg is more effective than granisetron 1 mg and ondansetron 4 mg in preventing PONV.
Aprepitant was significantly more effective than ondansetron for preventing vomiting at 24 and 48 hours after surgery and in reducing nausea severity in the first 48 hours after surgery. It also has a greater antiemetic effect compared with ondansetron. When used in combination, aprepitant 40 mg per os, plus dexamethasone, is more effective than ondansetron plus dexamethasone in preventing POV in patients undergoing craniotomy. A dose-ranging study for gynecologic laparotomy patients found a 80 mg per os dose of aprepitant is the most appropriate dose and is more effective than a 40 mg dose.
Preoperative dexamethasone 8 mg enhances the postdischarge quality of recovery in addition to reducing nausea, pain, and fatigue. Dexamethasone also has dose-dependent effects on quality of recovery. At 24 hours, patients receiving dexamethasone 0.1 vs 0.05 mg/kg required less opioid and reported less nausea, sore throat, muscle pain, and difficulty falling asleep. A meta-analysis evaluating the dose-dependent analgesic effects of perioperative dexamethasone found that doses >0.1 mg/kg are an effective adjunct in multimodal strategies to reduce postoperative pain and opioid consumption.
A recent meta-analysis suggests that with prophylactic low-dose droperidol (<1 mg or 15 µg/kg IV) in adults, there is still significant antiemetic efficacy with a low risk of adverse effects.
When haloperidol 1 mg was compared with ondansetron 4 mg and placebo, there was no difference in QTc effect among the 3 groups. There was no difference in PONV incidence between haloperidol and ondansetron given before the end of surgery, but both were not significantly better than placebo at 24 hours. There was no difference in early antiemetic efficacy between haloperidol 1 mg and ondansetron 4 mg and no difference in the risk of QT prolongation. Comparing haloperidol 2 mg IV vs ondansetron 4 mg IV given before the end of surgery, there was no difference in effect on early versus late PONV or QTc prolongation. However, Meyer-Massetti et al. recently reviewed the literature and all FDA Med Watch reports of haloperidol-associated adverse events and recommended doses of haloperidol <2 mg to reduce the risk of side effects and QT prolongation.
Meclizine 50 mg per os plus ondansetron 4 mg IV is more effective than either ondansetron or meclizine alone.
Scopolamine patch can be applied the evening before surgery or 2 to 4 hours before the start of anesthesia due to its 2- to 4-hour onset of effect. Adverse events associated with TDS are generally mild, the most common being visual disturbances, dry mouth, and dizziness.
Perphenazine is a phenothiazine derivative that has been used for the prevention of PONV at doses between 2.5 mg to 5 mg IV or IM.
Metoclopramide is a weak antiemetic and at a dose of 10 mg is not effective in reducing the incidence of nausea and vomiting. Metoclopramide in 25 and 50 mg doses had an effect similar to ondansetron 4 mg for early PONV but a smaller effect than ondansetron for late PONV. Dyskinesia or extrapyramidal symptoms were 0.6%, and 0.6%, respectively, and can increase with increasing metoclopramide doses.
Mirtazapine 30 mg per os plus dexamethasone 8 mg reduces the incidence of late PONV by >50% compared with dexamethasone 8 mg alone. Less rescue medication is needed with the combination of antiemetics.
Gabapentin doses of 600 mg per os given 2 hours before surgery effectively decreases PONV. Given 1 hours before surgery, gabapentin 800 mg per os is as effective as dexamethasone 8 mg IV, and the combination is better than either drug alone.
Midazolam 2 mg when administered 30 minutes before the end of surgery was as effective against PONV as ondansetron 4 mg.
The following strategies are not effective for PONV prophylaxis: music therapy, isopropyl alcohol inhalation, intraoperative gastric decompression, the proton pump inhibitor esomeprazole, and administration of nicotine patch 7 mg to nonsmokers. The latter modality may actually increase the incidence and severity of PONV. Although isopropyl alcohol inhalation is not effective for the prophylaxis of PONV, aromatherapy with isopropyl alcohol was effective in achieving a quicker reduction in nausea severity compared with promethazine or ondansetron when used for the treatment of PONV (Evidence A2).
A meta-analysis of 40 articles including 4858 subjects concluded that P6 stimulation with 10 different acupuncture modalities reduces nausea, vomiting, and the need for rescue antiemetics compared with sham stimulation (Evidence A1). The efficacy of P6 stimulation is similar to that of prophylactic antiemetics such as ondansetron, droperidol, metoclopramide, cyclizine, and prochlorperazine. In subgroup analysis, there was no difference in effectiveness in adults compared with children or invasive versus noninvasive modalities for P6 stimulation. The timing of transcutaneous acupoint electrical stimulation does not impact PONV, with similar reductions being achieved with stimulation initiated before or after induction of anesthesia. Neuromuscular stimulation over the median nerve also reduces the incidence of PONV in the early postoperative period, particularly when tetanic stimulation is used.
The additional costs associated with PONV in placebo patients are up to 100 times higher compared with prophylaxis with a generic antiemetic, and the cost of treating vomiting is 3 times higher than the cost of treating nausea. When using a willingness to pay rate of $100 per case avoided, PONV prophylaxis proved cost-effective in groups with a 40% risk of PONV. Lower drug acquisition costs would generally support PONV prophylaxis in patient groups at a lower risk for PONV. The decision about whether or not to use PONV prophylaxis, or to treat patients with established symptoms, not only depends on the efficacy of the drug but also on the baseline risk for PONV, adverse effects of the antiemetics, and drug acquisition costs, which will vary from 1 setting to another.
When nausea and vomiting occur postoperatively, treatment should be administered with an antiemetic from a pharmacologic class that is different from the prophylactic drug initially given, or if no prophylaxis was given, the recommended treatment is a low-dose 5-HT3 antagonist. During the first 4 postoperative hours, patients who failed PONV prophylaxis with ondansetron 4 mg did not respond either to a second administration of ondansetron 4 mg or to crossover with granisetron 0.1 or 1 mg.
The results show that mixing IV and per os antiemetics at various perioperative times decreases PDNV. For instance, 1 study found that dexamethasone 8 mg IV at induction plus ondansetron 4 mg IV at the end of surgery plus ondansetron 8 mg per os postoperatively had a greater effect on decreasing PDNV than ondansetron 4 mg IV alone at the end of surgery.
When developing a management strategy for each individual patient, the choice should be based on patient preference, C/E, and level of PONV risk. Among the interventions considered, a reduction in baseline risk factors and use of nonpharmacologic therapy are least likely to cause adverse events. PONV prophylaxis should be considered for patients at moderate to high risk for PONV. Depending on the level of risk, prophylaxis should be initiated with monotherapy or combination therapy using interventions that reduce baseline risk, nonpharmacologic approaches, and antiemetics. Antiemetic combinations are recommended for patients at moderate and high risk for PONV. When rescue therapy is required, the antiemetic should be chosen from a different therapeutic class than the drugs used for prophylaxis, and potentially one with a different mode of administration. If PONV occurs within 6 hours postoperatively, patients should not receive a repeat dose of the prophylactic antiemetic. An emetic episode more than 6 hours postoperatively can be treated with any of the drugs used for prophylaxis except dexamethasone, TDS, aprepitant, and palonosetron.
Category A: Supportive Literature
Randomized controlled trials report statistically significant (P < 0.01) differences between clinical interventions for a specified clinical outcome.
Level 1: The literature contains multiple randomized controlled trials, and aggregated findings are supported by meta-analysis.
Level 2: The literature contains multiple randomized controlled trials, but the number of studies is insufficient to conduct a viable meta-analysis for the purpose of these guidelines.
Level 3: The literature contains a single randomized controlled trial.
Methadone for perioperative pain #methadone #pain #ERAS
There’s a lot of great data that methadone use decreases postoperative narcotics use in cardiac surgery patients, and I believe it would really be a beneficial drug in an ERAS pathway for early extubation, decreased LOS in ICU and hospital, and better patient satisfaction. Please see the articles below/attached for references.
OVERALL: A variety of doses have been used in clinical trials, ranging from 0.1 to 0.3 mg/kg, with the majority of studies using a dose of either 0.2 mg/kg or a fixed dose of 20 mg.
Cardiac: Ketamine current pt weight (non-adjusted) 0.2mg/kg/hr start after induction (after lines placed) + 0.35 mg/kg 5-10 minutes prior to incison. Change from 0.2mg/kg/hr to 0.1mg/kg/hr when rewarming. Infusion off when driving sternal wires. Methadone currently not available.
Non-cardiac (cases 2+ hours duration) Ketamine: 0.3mg/kg (non-adjusted, current weight) at induction. Methadone currently not available.
Outpatient: ketamine not currently available for use.
July 2020
Cardiac: Ketamine IBW 0.3mg/kg total: 0.2mg/kg prior to incision + 0.1mg/kg when separate from CPB
0.2 mg/kg of methadone (based on ideal body weight, up to a maximal dose of 20 mg)
250 mg of ketamine was added to the dextrose 5% in water bag (total volume 500 ml). 500 ml bags were connected to a pump that was programed to deliver an infusion of ketamine dosed at ideal body weight (or an equal volume of dextrose 5% in water) at a rate of 0.3 mg · kg−1 · h−1 from induction of anesthesia until surgical closure, at which time the infusion was decreased to 0.1 mg · kg−1 · h−1. The infusion was maintained at a rate of 0.1 mg · kg−1 · h−1 in the postanesthesia care unit (PACU) and for the next 48 postoperative hours. Dosing of ketamine was based on recommendations in the literature17,18 and from clinical experience at our institution.
I have been utilizing ERAS in general surgery, OB, and ortho cases. Diving into one of my more tricky populations, I opted to see what ERAS practices are out there for cardiac surgery. Careful what you look for my friends. There’s actually a good amount of information out there!
Tranexamic acid or epsilon aminocaproic acid should be administered for on-pump cardiac surgical procedures to reduce blood loss.
Perioperative glycemic control is recommended (BS 70-180; [110-150]).
A care bundle of best practices should be performed to reduce surgical site infection.
Goal-directed therapy should be performed to reduce postoperative complications.
A multimodal, opioid-sparing, pain management plan is recommended postoperatively
Persistent hypothermia (T<35o C) after CPB should be avoided in the early postoperative period. Additionally, hyperthermia (T>38oC) should be avoided in the early postoperative period.
Active maintenance of chest tube patency is effective at preventing retained blood syndrome.
Post-operative systematic delirium screening is recommended at least once per nursing shift.
An ICU liberation bundle should be implemented including delirium screening, appropriate sedation and early mobilization.
Screening and treatment for excessive alcohol and cigarette smoking should be performed preoperatively when feasible.
Level IIa (Class of recommendation=Moderate Benefit)
Biomarkers can be beneficial in identifying patients at risk for acute kidney injury.
Rigid sternal fixation can be useful to reduce mediastinal wound complications.
Prehabilitation is beneficial for patients undergoing elective cardiac surgery with multiple comorbidities or significant deconditioning.
Insulin infusion is reasonable to be performed to treat hyperglycemia in all patients in the perioperative period.
Early extubation strategies after surgery are reasonable to be employed.
Patient engagement through online or application-based systems to promote education, compliance, and patient reported outcomes can be useful.
Chemical thromboprophylaxis can be beneficial following cardiac surgery.
Preoperative assessment of hemoglobin A1c and albumin is reasonable to be performed.
Correction of nutritional deficiency, when feasible, can be beneficial.
Level IIb (Class of recommendation=Weak Benefit)
A clear liquid diet may be considered to be continued up until 4 hours before general anesthesia.
Carbohydrate loading may be considered before surgery.
The Food and Drug Administration approved alvimopan in 2008 as an oral, peripherally acting opioid μ-receptor antagonist to accelerate GI recovery in patients undergoing bowel resection.87,88 A pooled analysis of 3 prospective randomized trials demonstrated that a 12 mg dosing regimen provided optimal reduction in GI morbidity and return of GI function after abdominal surgery.89
Vaughan-Shaw et al90 performed a meta-analysis involving 3 studies of 1388 patients undergoing open abdominal surgery (bowel resection and hysterectomy) within a defined accelerated recovery program. This study demonstrated a 16- to 20-hour reduction in the time to GI recovery and discharge order associated with alvimopan use. It is important to note that the defined accelerated recovery program in each of these studies was limited to early removal of prophylactic NG tubes, clear liquids on POD 1, and encouragement of ambulation. Each study utilized patient-controlled analgesia with heavy doses of opioids.91 Therefore, these trials were conducted in open surgery within the setting of an opioid-centric treatment pathway, which is not consistent with most modern day ERPs. There are no high-quality prospective randomized trials examining the efficacy of alvimopan within the setting of an opioid-restricted modern day ERP or after minimally invasive surgery.
However, there are large database studies evaluating the use of alvimopan in current practice. The Michigan Surgical Quality Collaborative group reported that the usage of alvimopan in the community resulted in a decrease in mean LOS (4.8 vs 6.4 days) due principally to a reduction in ileus (7.9% vs 2.3%).92 Similarly, the Surgical Care and Outcomes Assessment Program evaluated 14,781 patients undergoing elective CRS comparing those that did (11%) and did not receive (89%) alvimopan and found a LOS reduction of 1.8 days and a cost reduction of $2017 related to ileus reduction in patients receiving alvimopan.93 Adam et al94 reported on a single institution experience of 660 patients after implementation of alvimopan as part of an established ERP (197 alvimopan; 463 no alvimopan) and demonstrated a faster return of bowel function, a lower incidence of ileus, a shorter LOS, and a hospital cost savings of $1492 per patient. These results are consistent with similar retrospective cohort study by Itawi et al.95 It should be noted that the potential benefits of alvimopan are likely related to the amount/duration of opioid analgesics as demonstrated by 2 separate retrospective studies demonstrating minimal benefit in a laparoscopic colectomy population managed with minimal opioids.96,97
The data suggest a reproducible benefit associated with the use of alvimopan in open CRS; however, the cost/benefit ratio must be considered within the context of the opioid administration of each institution’s ERP. Barletta et al50 confirmed that the intravenous opioid dosage that results in ileus might be quite modest (2-mg hydromorphone). Additional data would be helpful to clearly define the minimum dose exposure and route of administration of opioids that would best guide the use of alvimopan within a comprehensive ERP. However, if modest opioid exposure is anticipated, the agent appears to be cost-effective.