It seems that ever since that advent of dexmedetomidine, propofol has been pushed aside as the sedation drug of choice for sedation during and post-open heart surgery. But is the literature changing with the effects of dexmedetomidine on rates of atrial fibrillation?
In patients older than 60 years with low baseline risk of postoperative delirium admitted to the ICU after cardiac surgery and extubated within 12 h of ICU admission, a post-extubation nighttime dose of dexmedetomidine may reduce the incidence of delirium on postoperative day one.
The study results showed no statistically significant difference between both groups with regard to age and body mass index. Group P patients were more associated with lower MAP and HR than Group D patients. There was no statistically significant difference between groups with regard to ABG findings, oxygenation, ventilation, and respiratory parameters. There was significant difference between both the groups in midazolam and fentanyl dose requirement and financial costs with a value of P < 0.05.
Meta-analysis studies on the use of DEX during cardiac surgery also showed a reduction in the risk of atrial fibrillation, ventricular tachycardia and cardiac arrest [7, 12].
Our findings suggest that DEX may reduce short term postoperative pulmonary complications, time on mechanical lung ventilation, ICU and hospital stay following CABG surgery compared to propofol.
When compared with propofol, dexmedetomidine sedation reduced incidence, delayed onset, and shortened duration of POD in elderly patients after cardiac surgery. The absolute risk reduction for POD was 14%, with a number needed to treat of 7.1.
Dexmedetomidine did not significantly impact ICU length of stay compared with propofol, but it significantly reduced the duration of mechanical ventilation and the risk of delirium in cardiac surgical patients. It also significantly increased the risk of bradycardia across ICU patient subsets.
The use of dexmedetomidine for sedation after cardiac surgery was associated with a lower incidence of atrial fibrillation and hence decreased the duration of intensive care stay.
This trial demonstrated that dexmedetomidine sedation may be better able to improve microcirculation in cardiac surgery patients during the early postoperative period compared with propofol.
Adding low-dose rate dexmedetomidine to a sedative regimen based on propofol did not result in a different risk of in-hospital delirium in older patients undergoing cardiac surgery. With a suggestion of both harm and benefit in secondary outcomes, supplementing postoperative propofol with dexmedetomidine cannot be recommended based on this study.
Dexmedetomidine infusion, started at anaesthetic induction and continued for 24 h, did not decrease postoperative atrial arrhythmias in patients recovering from cardiac surgery. Dexmedetomidine also worsened delirium, although not by a significant amount, possibly by provoking hypotension. Dexmedetomidine worsened kidney injury, but again not by a significant amount. The incidence of persistent surgical pain was similar in each group. Dexmedetomidine should be used cautiously in cardiac surgical patients with attention to preventing hypotension, and should not be given in expectation of reducing atrial fibrillation or delirium.
Dexmedetomidine-based sedation resulted in achievement of early extubation more frequently than propofol- based sedation. Mean postoperative time to extubation and average hospital LOS were shorter with dexmedetomidine- based sedation and met a statistical level of significance. There was no difference in ICU-LOS or in-hospital mortality between the two groups. Total hospital charges were similar, although slightly higher in the propofol group.
In the massively bleeding patient with coagulopathy, our group recommends the administration of an initial bolus of 25 IU.kg-1. This applies for: the acute reversal of vitamin K antagonist therapy; haemostatic resuscitation, particularly in trauma; and the reversal of direct oral anticoagulants when no specific antidote is available.
In patients with a high risk for thromboembolic complications, e.g. cardiac surgery, the administration of an initial half-dose bolus (12.5 IU.kg-1) should be considered.
A second bolus may be indicated if coagulopathy and microvascular bleeding persists and other reasons for bleeding are largely ruled out. Tissue-factor-activated, factor VII-dependent and heparin insensitive point-of-care tests may be used for peri-operative monitoring and guiding of prothrombin complex concentrate therapy.
For the endpoint of rapid INR reduction, the results from our trial are consistent with previously published (mainly observational) data and demonstrate that 4F-PCC is non-inferior and superior to plasma for rapid INR reduction in patients on VKA therapy.
Furthermore, we noted that 4F-PCC could be given more rapidly than plasma, which is in agreement with previously published (retrospectively collected) data.24
For the endpoint of clinical efficacy, we found no other adequately powered trial examining reversal of VKA therapy in patients needing urgent surgical procedures, and this trial therefore offers new insights into their treatment. We noted that 4F-PCC was superior to plasma for haemostatic efficacy.
Although our study was not powered to assess safety, we did not detect any between-treatment differences for the occurrence of thromboembolic events or deaths, a finding in agreement with the existing scientific literature.11, 17, 25, 26 Additionally, although these data guide clinicians on how best to achieve urgent VKA reversal, the scientific literature concerning which patients should be urgently reversed before surgical or invasive interventions continues to evolve; for example, findings from a recent trial showed the safety of pacemaker placement without interruption of anticoagulation.29
Among the key recommendations in this article are the following:
For dosing of VKAs, we recommend the initiation of oral anticoagulation therapy, with doses between 5 mg and 10 mg for the first 1 or 2 days for most individuals, with subsequent dosing based on the international normalized ratio (INR) response (Grade 1B); we suggest against pharmacogenetic-based dosing until randomized data indicate that it is beneficial (Grade 2C); and in elderly and other patient subgroups who are debilitated or malnourished, we recommend a starting dose of ≤ 5 mg (Grade 1C). The article also includes several specific recommendations for the management of patients with nontherapeutic INRs, with INRs above the therapeutic range, and with bleeding whether the INR is therapeutic or elevated.
For the use of vitamin K to reverse a mildly elevated INR, we recommend oral rather than subcutaneous administration (Grade 1A).
For most patients who have a lupus inhibitor, we recommend a therapeutic target INR of 2.5 (range, 2.0 to 3.0) [Grade 1A].
We recommend that physicians who manage oral anticoagulation therapy do so in a systematic and coordinated fashion, incorporating patient education, systematic INR testing, tracking, follow-up, and good patient communication of results and dose adjustments [Grade 1B].
In patients who are suitably selected and trained, patient self-testing or patient self-management of dosing are effective alternative treatment models that result in improved quality of anticoagulation management, with greater time in the therapeutic range and fewer adverse events. Patient self-monitoring or self-management, however, is a choice made by patients and physicians that depends on many factors. We suggest that such therapeutic management be implemented where suitable (Grade 2B).
In patients on VKA therapy presenting with severe hemorrhage, international guidelines recommend, as soon as the diagnosis is confirmed, the administration of PCC (≥20 UI/kg) and vitamin K (≥5 mg) to normalize coagulation (post-reversal INR ≤1.5).
A guideline-concordant administration dose of PCC and vitamin K administrated in the first eight hours was associated with a two-fold decrease in seven-day mortality overall and with a three-fold decrease in the ICH subgroup
The guideline-concordant reversal was performed in 38% of the patients within eight hours after admission
Whereas pre-reversal INR is not absolutely necessary, post-reversal INR is essential to evaluate treatment efficacy
The post-reversal INR target must be performed systematically and immediately after PCC administration
Healthy appearing patient with afib s/p ablation and returning for repeat ablation for recurrent afib. Anesthesia induced normally and patient VSS. 3 minutes after a request of a heparin bolus, patient dropped their SBP into the upper 40s, lower 50s. Patient recovered well after small bolus of epinephrine. ICE used to rule out pericardial effusion as well as confirm normal LVEF and RVEF.
What does an angiotensin receptor blocker (ARB) do?
Angiotensin II receptor blockers (ARBs) represent a newer class of effective and well tolerated antihypertensive agents 1. Several clinical studies have indicated the beneficial effects of ARBs in hypertensive patients such as reduction of left ventricular hypertrophy, decrease in ventricular arrhythmias, and improved diastolic function 1. Inhibitors of the renin-angiotensin system (RAS), either angiotensin converting enzyme (ACE) inhibitors or ARBs, mediate vasodilation and consequently decrease blood-pressure by different mechanisms 1. ARBs specifically inhibit angiotensin II from binding to its receptor, the Angiotensin-1 (AT 1) receptor on vascular smooth muscle cells. This blockade results in increased angiotensin II and normal bradykinin plasma levels. ARBs were developed to overcome several deficiencies of ACE inhibitors, which, by comparison, lead to decreased angiotensin II, but increased bradykinin levels. Hence, the key advantage of ARBs over ACE inhibitors is their lack of adverse effects related to bradykinin potentiation. ARBs have been shown to reduce morbidity and mortality associated with hypertension, and therefore, it is not surprising that an increasing number of patients scheduled for surgery are chronically treated with ARBs 2. However, RAS blockade increases the risk of severe hypotension during and after anesthetic induction. ACE-inhibitors are well known for inducing severe circulatory side effects during anesthesia, which led to the general recommendation to withhold the drug on the day of surgery 3.
Chronic AT 1 blockade also reduces the vasoconstrictor response to α 1 receptors activated by norepinephrine, which explains why ARB-induced hypotension can be so resistant to phenylephrine, ephedrine and norepinephrine 2, 8 Clinical studies have shown significant vasoconstrictor effects of vasopressin and increased cardiac filling during echocardiographic measurements 2.
Vasopressin or its synthetic analogues can restore the sympathetic response and may be useful pressors in cases of refractory hypotension during anaphylaxis 9 and septic shock 10 as well as in patients on RAS inhibitors, although norepinephrine has been reported to have a more favorable effect on splanchnic perfusion and oxygen delivery 11.
When conventional therapies such as: decreasing the anesthetic agent, volume expansion, phenylephrine, ephedrine, norepinephrine, and epinephrine are not effective, exogenous vasopressin may improve hypotension. To date, at least 5 clinical trials have demonstrated that patients on chronic ACEI/ARB undergoing general anesthesia, respond to exogenous vasopressin derivatives with an increase in blood pressure and fewer hypotensive episodes.6,7 Typically, a 0.5-1 unit bolus of AVP is administered to achieve a rise in mean arterial pressure.4 The subsequent recommended infusion dose is 0.03U/min for AVP and 1-2 mcg/kg/h for terlipressin. Caution should be used as V1 agonists have been associated with the following deleterious effects: reduction in cardiac output and systemic oxygen delivery, decreased platelet count, increased serum aminotransferases and bilirubin, hyponatremia, increased pulmonary vascular resistance, decrease in renal blood flow, increase in renal oxygen consumption, and splanchnic vasoconstriction.
Studies involving cardiac surgical patients suggest that MB treatment for patients with VS may reduce morbidity and mortality.5 It has also been suggested that the early use (preoperative use in patients at risk for VS) of MB in patients undergoing coronary artery bypass grafting may reduce the incidence of VS.5,9A bolus dose of 1-2mg/kg over 10-20 minutes followed by an infusion of 0.25mg/kg/hr for 48-72 hours is typically utilized in clinical practice and trials (with a maximum dose of 7 mg/kg).10 Side effects include cardiac arrhythmias (transient), coronary vasoconstriction, increased pulmonary vascular resistance, decreased cardiac output, and decreased renal and mesenteric blood flow.1 Both pulse and cerebral oximeter readings may not be reliable during MB administration due to wavelength interference.11,12 The use of MB is absolutely contraindicated in patients with severe renal impairment because it is primarily eliminated by the kidney.13 It may also cause methemoglobinemia and hemolysis.13 At high doses, neurotoxicity may occur secondary to the generation of oxygen free radicals. Neurologic dysfunction may be more severe in patients receiving serotoninergic agents such as: tramadol, ethanol, antidepressants, dopamine agonists and linezolid. Recommended doses for VS ranging from 1-3 mg/kg do not typically cause neurologic dysfunction.14 However, recent reports suggest that MB in doses even ≤ 1mg/kg in patients taking serotonin reuptake inhibitors (SSRIs) may lead to serotonin toxicity due to its monoamine oxidase (MAO) inhibitor property.15
Over the years, our hospital has been using Amicar… until there was a drug shortage. With that drug shortage came a different drug called tranexamic acid. We’ve been using it for awhile and I can’t seem to tell a difference in coagulation between the two drugs. Let’s break down each one and also discuss cost-effectiveness.
Tranexamic acid acts by reversibly blocking the lysine binding sites of plasminogen, thus preventing plasmin activation and, as a result, the lysis of polymerised fibrin.12 Tranexamic acid is frequently utilised to enhance haemostasis, particularly when fibrinolysis contributes to bleeding. In clinical practice, tranexamic acid has been used to treat menorrhagia, trauma-associated bleeding and to prevent perioperative bleeding associated with orthopaedic and cardiac surgery.13–16 Importantly, the use of tranexamic acid is not without adverse effects. Tranexamic acid has been associated with seizures,17 18 as well as concerns of possible increased thromboembolic events, including stroke which to date have not been demonstrated in randomised controlled trials.
Fibrinolysis is the mechanism of clot breakdown and involves a cascade of interactions between zymogens and enzymes that act in concert with clot formation to maintain blood flow.25 During extracorporeal circulation, such as cardiopulmonary bypass used in cardiac surgery, multiplex changes in haemostasis arise that include accelerated thrombin generation, platelet dysfunction and enhanced fibrinolysis.26 Tranexamic acid inhibits fibrinolysis, a putative mechanism of bleeding after cardiopulmonary bypass, by forming a reversible complex with plasminogen.
In summary, we found no evidence that tranexamic acid increases the risk of death and thrombotic complications after coronary-artery surgery. Tranexamic acid was associated with a lower risk of bleeding complications than placebo but also with a higher risk of postoperative seizures.
The study used a high-dose regimen, in which either 50 mg/kg or 100 mg/kg of TXA was delivered for each patient. There is a possibility that lower dose of TXA can be equally effective while causing less adverse effects. In fact, TXA plasma concentrations required to suppress fibrinolysis and plasmin-induced platelet activation are merely 10 and 16 μg/ml, respectively [7, 8]. This relatively low plasma concentration can be reached in cardiac surgery when 10 mg/kg of TXA is administered as a bolus then followed by continuous infusion of 1 mg kg/h and 1 mg/kg in CPB [9]. But another potential mechanism of TXA action might be the increase in thrombin formation, which requires concentrations more than 126 μg/ml to be effective [10, 11]. 30 mg/kg of TXA administered as a bolus followed by 16 mg/kg/h and 2 mg/kg in CPB prime solution was able to maintain the plasma concentration above 114 μg/ml [9].
Using their model-based meta-analysis, the authors conclude that low-dose tranexamic acid (total dose of 20 mg/kg of actual body weight) provides the best balance between reduction in postoperative blood loss and red blood cell transfusion and the risk of clinical seizure. The use of higher doses would only marginally improve the clinical effect at the cost of an increased risk of seizure.
Low-risk group received a single 50 mg/kg TXA bolus after induction of anesthesia. The high-risk group received Blood Conservation Using Anti-fibrinolytics Trial (BART) TXA regimen, consisting of 30 mg/kg bolus infused over 15 minutes after induction, followed by 16 mg/kg/h infusion until chest closure with a 2 mg/kg load within the pump prime.
Risk of seizure is dose-dependent, with the greatest risk at higher doses of tranexamic acid. We conclude that, in general, patients with a high risk of bleeding should receive high-dose tranexamic acid, while those at low risk of bleeding should receive low-dose tranexamic acid with consideration given to potential dose-related seizure risk. We recommend the regimens of high-dose (30 mg kg−1 bolus + 16 mg kg−1 h−1 + 2 mg kg−1 priming) and low-dose (10 mg kg−1 bolus + 1 mg kg−1 h−1 + 1 mg kg−1 priming) tranexamic acid, as these are well established in terms of safety profile and have the strongest evidence for efficacy.
The exposure value with the low-dose tranexamic acid regimen proposed by Horrow et al. (10 mg/kg followed by 1 mg/kg/h over 12 h) was close to the 80% effective concentration for postoperative blood loss and above the 80% effective concentration for erythrocyte transfusion. Compared to this regimen, a fivefold increase in total dose (100 mg/kg) achieved only a 58 ml (95% credible interval,54 to 65 ml) increment in the reduction of postoperative blood loss, up to 48 h postsurgery, with a decrease in erythrocyte transfusion rate from 46% to 44%.
Concentrations close to 80% effective concentration can be achieved at the end of surgery with a low-dose regimen administered either as a preoperative bolus plus infusion (10mg/kg followed by 1mg/kg/h) or as a single preoperative loading dose of 20mg/kg (fig. 6). Postoperative administration of tranexamic acid appears unnecessary because tranexamic acid concentrations will decrease but nevertheless remain sufficient (greater than or equal to EC50) up to the end of the drug’s contribution to blood loss reduction (8 h after the start of surgery).
The type of surgery and the duration of CPB both affected the risk of seizure. Open-chamber surgery resulted in a 5.5-fold increase in the risk of seizure compared to closed-chamber procedures (95% credible interval, 3.2 to 10). Each additional hour of CPB doubled the risk of seizure (2.0;95% credible interval, 1.2 to 3.2).
Ortho/Spine
OB
Trauma
Currently at our hospital (June 2022):
TXA DOSING AND ADMINISTRATION OVERVIEW
How supplied from Pharmacy
TXA 1000mg/10mL vials Will not provide premade bags like with Amicar; Amicar is a more complex mixture than TXA Will take feedback on this after go-live and reassess
There are a number of dosing strategies in the literature. What I recommend for maximal safety and efficacy is taken from Zuffery, et al. Anesthesiology 2021 meta-analysis and is practiced at Scripps Mercy.
~ 20 mg/kg total dose recommended in this meta-analysis.
Two dosing strategies they report that were as effective as high-dose but with lower seizure risk than high dose:
Carrie our pharmacist provided some really helpful research and updates:
So really we have two questions here I am seeking to answer with your group: (1) Is TXA best given as a bolus or as an infusion during cardiac surgery, and my other question (2) What is the optimal TXA dosage?
The JAMA 2022 study focuses on the question of dosing, though I believe it also helps answer the question about continuing drips post-op.
In this study, they did a bolus/infusion but only during the surgery.
They performed a randomized double-blind trial of 2 different TXA dosing strategies for adults undergoing cardiac surgery with CPB. They two dosing strategies:
“High dose”: TXA 30mg/kg bolus followed by 16mg/kg/h during surgery only and 2mg/kg pump prime
“Low dose”: TXA 10mg/kg bolus followed by 10mg/kg/h during surgery only and 1mg/kg pump prime
Results:
Efficacy: 21.8% of patients in the high-dose group received at least 1 allogeneic RBC transfusion compared to 26.0% in the low-dose group (p=0.004).
Safety: The composite safety endpoint (seizure, kidney dysfunction, thrombotic events, and all-cause mortality) was 17.6% in high-dose vs 16.8% in low-dose (p=0.004 for noninferiority)
I like this infographic on their study and results:
My takeaway on the JAMA study: I’m not sold on the “high dosing” regimen because I’m not overly impressed by their efficacy endpoint. Transfusion of at least 1 PRBC by itself doesn’t say much (in my opinion – let me know what you think!). Transfusion of FFP, platelets, cryo were no different between dosing groups. Chest tube output was not statistically different post-op. Duration of mechanical ventilation, ICU length of stay, and hospital length of stay were not statistically different.
Furthermore, if you comb through their secondary safety endpoints, you can see where TXA “low dose” patients had lower rates of seizures compared to high dose. This was especially true for open chamber surgery.
This doesn’t answer the question you asked about dosing strategy – bolus versus drip. However, they did only run TXA intraoperatively and did NOT give it post-op, which at least supports the idea we don’t need it upon ICU transfer.
I’m in favor of us moving toward the above JAMA “low dose” strategy among our anesthesiologists who are running drips. I think we can actually increase the rate of the infusion and STOP it before patient transfers, because at that point TXA will have already done all the leg work it is going to do.
Okay, so back to the question on bolus versus infusion:
I really like their Figure 6, where they show pharmacokinetics and outcomes based on four different TXA regimen simulations. You can see where TXA 20mg/kg bolus (represented with yellow) is pretty similar outcomes and PK-wise to the green 10mg/kg bolus followed by 1mg/kg/h for 12 hours. AKA what you’re doing vs. what most of your colleagues are doing – same outcomes represented in this simulation.
“The following tranexamic acid regimens were simulated: 100 mg/kg preoperative loading dose (blue dashed line and blue triangle); 30 mg/kg preoperative loading dose followed by 16 mg · kg–1 · h–1 during surgery with a further 2 mg/kg added to the cardiopulmonary bypass (CPB) pump prime (red solid line and red triangle for 3 h of surgery, red circle for 4 h of surgery); 10 mg/kg preoperative loading dose followed by 1 mg · kg–1 · h–1 for 12 h (green solid line and green circle); 20 mg/kg preoperative loading dose (yellow dashed line and yellow triangle). Top left, Predicted concentrations of tranexamic acid for various regimens indicated as described above, the dark gray column representing the mean duration of CPB in the meta-analysis. Top right, Predicted postoperative mediastinal blood loss without tranexamic acid (gray solid line) and for the different tranexamic acid regimens indicated as described above. Bottom, As a function of the mean tranexamic acid concentration from start of surgery up to 12 h, the probability of erythrocyte transfusion (left) and of seizure (right). Bottom right, The black solid line represents model-based study-level predictions of a hypothetical trial of patients undergoing coronary artery bypass grafting with a mean duration of surgery and CPB of 3 h and 1.5 h, respectively; the black dot-dash line represents model-based predictions at the study level of a hypothetical trial in patients undergoing open-chamber surgery with a mean duration of surgery and CPB of 4 h and 2.5 h, respectively; the average weight was 74 kg.”
This NEJM RCT from 2017 from Myles, et al studied 50mg/kg and dosed as follows : “30-min loading dose of 12.5 mg/kg with a maintenance infusion of 6.5 mg/kg/hr, and 1 mg/kg added to the CPB prime, will be used” > Infusions again, but intraop only. This study also started with giving 100 mg/kg!! Patients were seizing, so they pulled back 50mg/kg.
My plan:
TXA 20mg/kg over 20 minutes prior to incision + 2mg/kg in pump prime. No infusion.
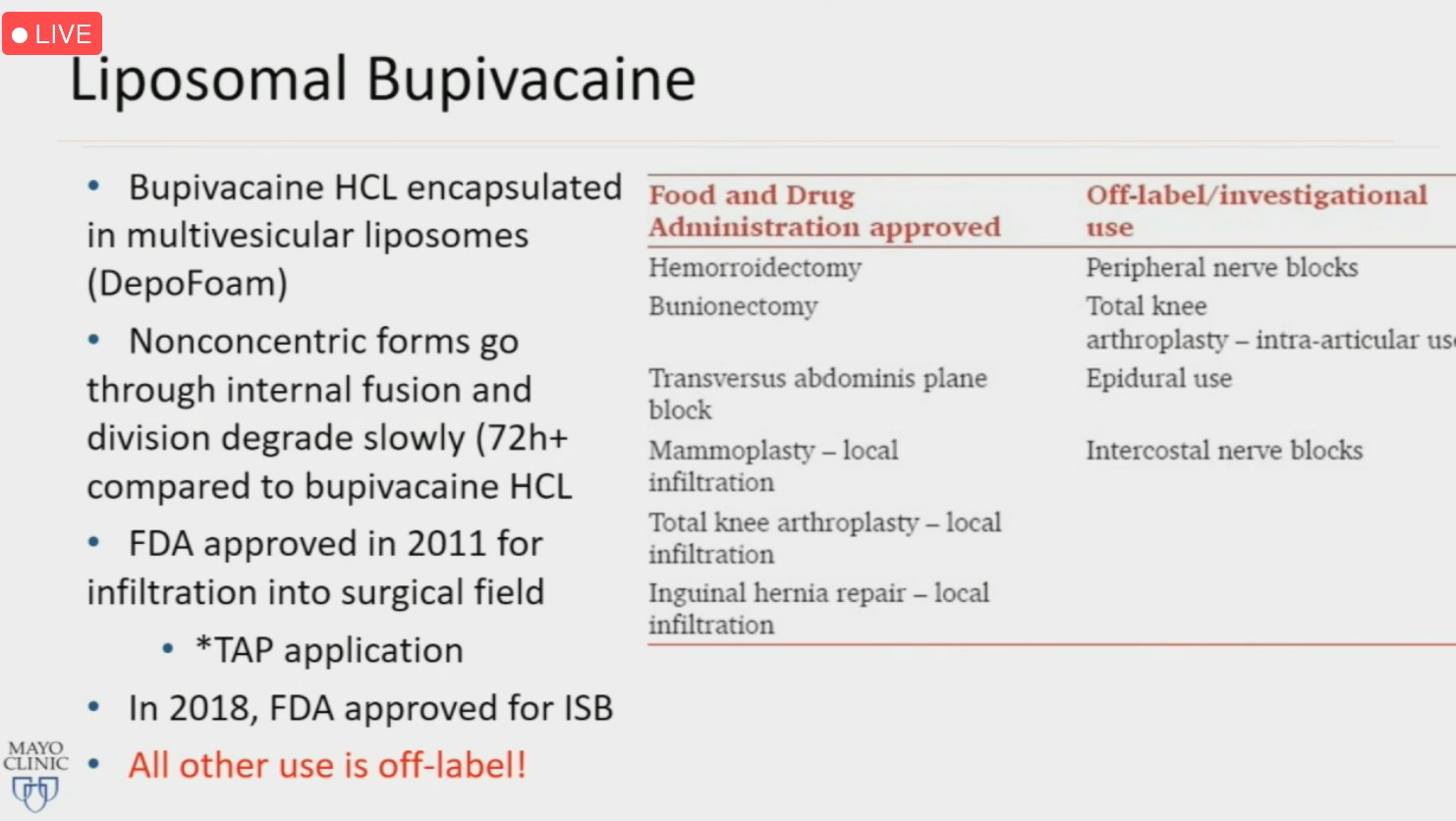
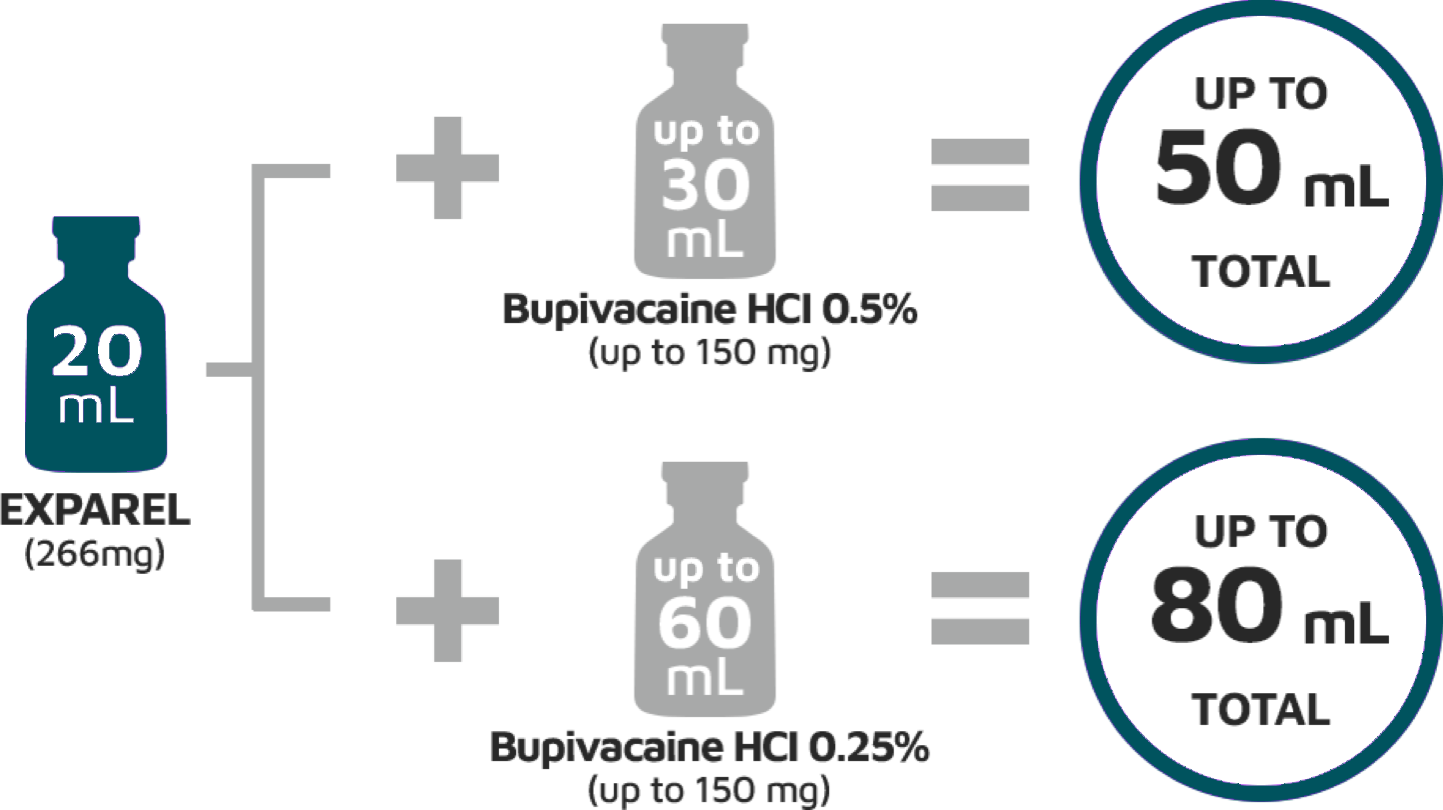
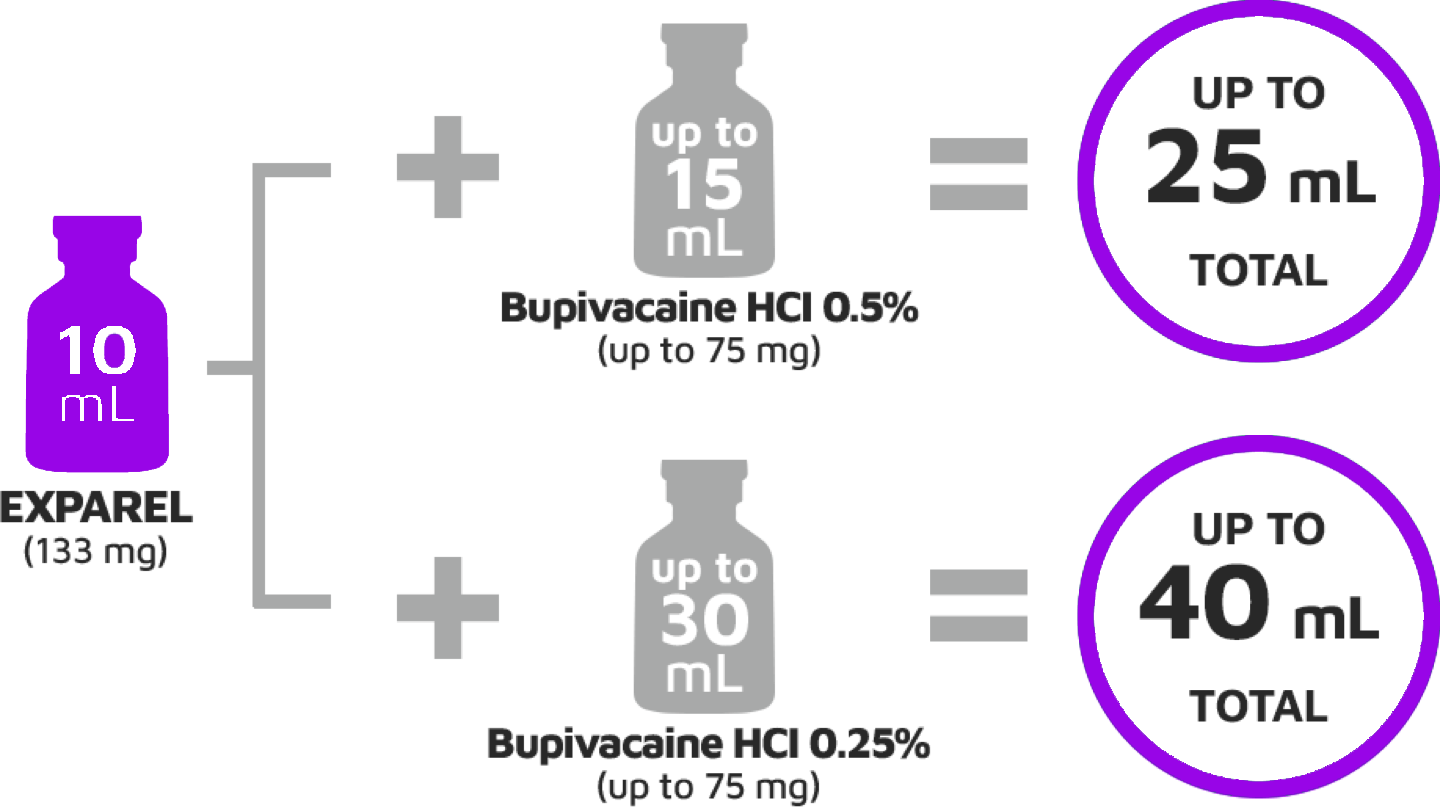
Liposomal bupivacaine (Exparel) is a longer acting form of traditional bupivacaine that delivers the drug by means of a multivesicular liposomal system.
VATs: Dilute liposomal bupivacaine (266 mg, 20 cc) mixed with 20 cc injectable saline. We use two syringes to save time (refill syringe between injections).
For planned thoracotomy, we add 60 cc injectable saline for wider injection.
The efficacy of this strategy requires attention to specific details, such as timing and technique of injection, dilution with saline, and injection of multiple interspaces (typically interspaces 3–10 when technically possible).
Inject EXPAREL slowly and deeply (generally 1-2 mL per injection) into soft tissues using a moving needle technique (ie, inject while withdrawing the needle)
Infiltrate above and below the fascia and into the subcutaneous tissue
Aspirate frequently to minimize the risk of intravascular injection
Use a 25-gauge or larger-bore needle to maintain the structural integrity of the liposomal particles
Inject frequently in small areas (1-1.5 cm apart) to ensure overlapping analgesic coverage
Patient safety is crucial for the delivery of effective, high-quality healthcare1 and is defined by the World Alliance for Patient Safety of WHO as ‘the reduction of risk of unnecessary harm associated with healthcare to an acceptable minimum’. The practice and delivery of healthcare is argued to be fundamentally and critically dependent on effective and efficient communication. Depending on physicians’ needs and responsibilities, handoff content will vary, requiring customization by individual physician groups; there is no “one size fits all” content.