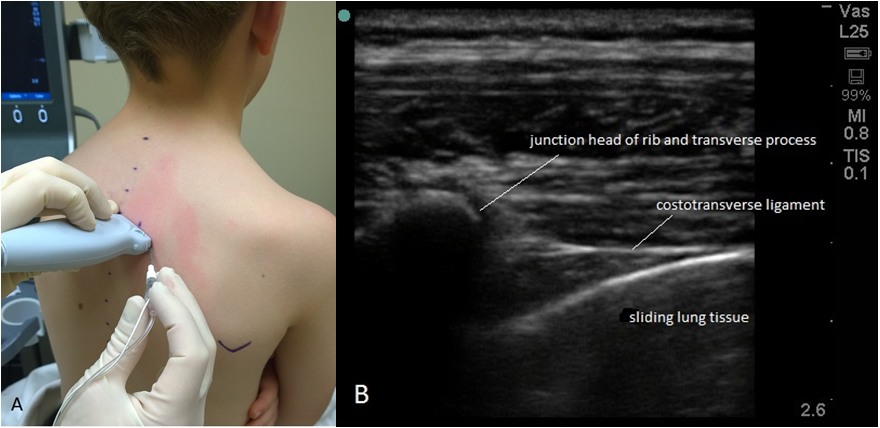
To place the PV catheter at the T4-5 level, the authors used an in-plane transverse technique under ultrasound guidance, with the probe in a transverse orientation. After identifying the anatomic landmarks on ultrasound, a 17-gauge Tuohy needle was advanced in a lateral to medial direction, until the tip was beneath the transverse process. For all recipients in the study, the authors further confirmed correct PV catheter placement with real-time infusion of a local anesthetic (1-3 mL of 1.5% lidocaine with epinephrine 1:200,000); they were able to visualize on ultrasound the spread from the tip of the catheter.
Once it was confirmed that the tip remained in position, the PV catheter was secured with skin glue (Dermabond®, Ethicon, Inc.; Somerville, NJ). Next, at the PV catheter insertion site, the authors placed an occlusive dressing on a chlorhexidine-impregnated sponge (BioPatch®, Johnson & Johnson Wound Management, a division of Ethicon, Inc.; Somerville, NJ). The PV catheter was connected to an elastomeric pump (ON-Q®, Halyard Health, Alpharetta, GA), an infusion of 0.2% ropivacaine was started at a rate of 0.2 to 0.25 mL/kg/h; the maximum dose was 7 mL/h per side in bilateral lung transplant recipients and 14 mL/h in unilateral single-lung transplant recipients.
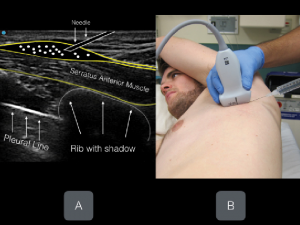
Under sterile conditions and while patients still were in the lateral position with the diseased side up, a linear ultrasound transducer (10-12 MHz) was placed in a sagittal plane over the midclavicular region of the thoracic cage. Then the ribs were counted down until the fifth rib was identified in the midaxillary line (Fig 1).18 The following muscles were identified overlying the fifth rib: the latissimus dorsi (superficial and posterior), teres major (superior), and serratus muscles (deep and inferior). The needle (a 22-gauge, 50-mm Touhy needle) was introduced in plane with respect to the ultrasound probe, targeting the plane superficial to the serratus anterior muscle (Fig 2). Under continuous ultrasound guidance, 30 mL of 0.25% levobupivacaine was injected, and then a catheter was threaded. A continuous infusion of 5 mL/hour of 0.125% levobupivacaine then was started through the catheter.
For my single shot blocks, I’m always looking for ways to prolong my regional anesthetic effect. For awhile, Exparel was the most talked about drug to have a 72 hour blockade. We don’t have this medication available to us at the hospital. Therefore, it’s time to get creative and hit the literature to see what has worked for prolonging our blocks.
Sensory block duration was prolonged by 150 min [95% confidence interval (CI): 96, 205, P,0.00001] with intrathecal dexmedetomidine. Perineural dexmedetomidine used in brachial plexus (BP) block may prolong the mean duration of sensory block by 284 min (95% CI: 1, 566, P¼0.05), but this difference did not reach statistical significance. Motor block duration and time to first analgesic request were prolonged for both intrathecal and BP block. Dexmedetomidine produced reversible bradycardia in 7% of BP block patients, but no effect on the incidence of hypotension. No patients experienced respiratory depression.
Considerable differences existed in the doses of perineural dexmedetomidine; doses varied between 3, 5, 10, or 15 mcg for the intrathecal route, and 30, 100, 0.75, 1 mcg/kg for the peripheral route.
Intravenous DEX at a dose of 2.0 μg/kg significantly increased the duration of ISBPB analgesia without prolonging motor blockade and reduced the cumulative opioid consumption at the first 24 hours in patients undergoing arthroscopic shoulder surgery.
30 ml of 0.325% bupivacaine + 1 ml (100 μg) dexmedetomidine were given for supraclavicular brachial plexus block using the peripheral nerve stimulator.
Below knee surgery under combined femoral-sciatic nerve block were randomly allocated into two groups to have their block performed using bupivacaine 0.5% alone (group B) or bupivacaine 0.5% combined with 100 μg bupivacaine-dexmedetomidine
Randomized to receive ISB using 15 ml ropivacaine, 0.5%, with 0.5 μg/kg dexmedetomidine administered perineurally (DexP group), intravenously (DexIV group), or none (control group). DexIV was noninferior to DexP for these outcomes. Both dexmedetomidine routes reduced the pain and opioid consumption up to 8 h postoperatively and did not prolong the duration of motor blockade.
After speaking to a colleague of mine regarding regional anesthesia for thoracotomy and mastectomy, I am reading up on Erector Spinae Plane (ESP) block.
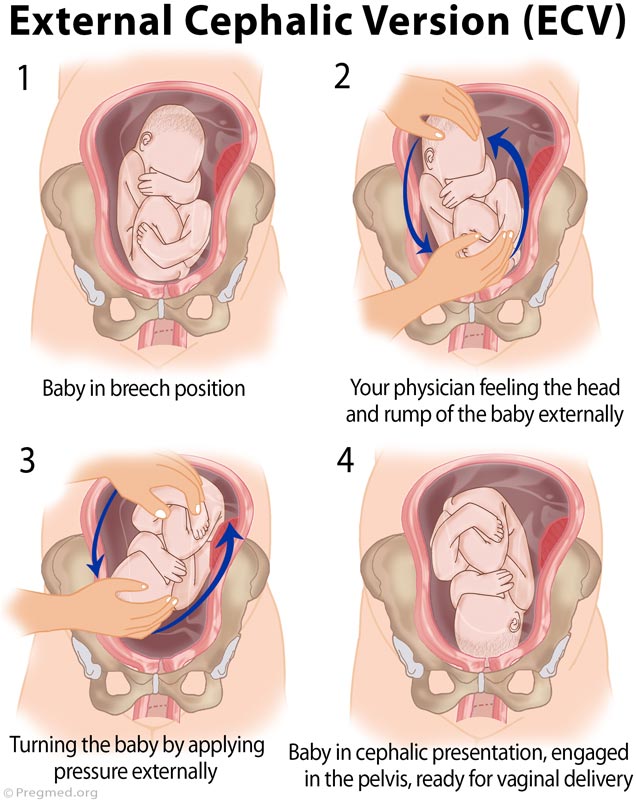
Conclusions: Spinal Anesthesia (SA: hyperbaric bupivacaine 9mg + fentanyl 15mcg) increased the success rate and reduced pain for both primary and re-attempts of External Cephalic Version (ECV), whereas IV Anesthesia (IVA) using remifentanil infusion (0.1mcg/kg/min) only reduced the pain. There was no significant increase in the incidence of fetal bradycardia or emergency CS, with ECV performed under anaesthetic interventions. Relaxation of the abdominal muscles from SA appears to underlie the improved outcomes for ECV.
Editor’s key points: There is no consensus on best anaesthetic technique for external cephalic version (ECV). In this study, success at ECV was higher using spinal anaesthesia compared with remifentanil infusion or no intervention. Pain was also reduced in the remifentanil group but success at ECV was no different to the no intervention group. The effect of spinal anaesthesia in ECV may relate to relaxation of the abdominal musculature.
Neuraxial blockade is associated with minimal hospital and insurer cost changes in the setting of external cephalic version, while reducing the cesarean delivery rate.
It is both effective and cost-effective to utilize spinal anesthesia to perform ECV in term, nulliparous women with breech fetuses. Translation of this potentially impactful approach into broad obstetric practice should be undertaken.
Six RCTs met criteria for study inclusion. Regional anesthesia was associated with a higher external cephalic version success rate compared to intravenous or no analgesia (59.7% vs. 37.6%; pooled RR 1.58, 95% confidence interval [CI] 1.29-1.93). This significant association persisted when the data was stratified by type of regional anesthesia (spinal vs. epidural). The number needed to treat with regional anesthesia to achieve one additional successful ECV was 5. There was no evidence of statistical heterogeneity (p=0.32, I2=14.9%) or publication bias (Harbord test p=0.78). There was no statistically significant difference in the risk of cesarean delivery comparing regional anesthesia to intravenous or no analgesia (48.4% vs. 59.3%; pooled RR 0.80, 95% CI 0.55-1.17). Adverse events were rare and not significantly different between the two groups.
Neuraxial Anesthesia (NA) for External Cephalic Version (ECV) increased the risk of emergent cesarean delivery (CD) without impacting ECV success. These findings differ from previous randomized controlled trials (RCTs). The increased risk and decreased success of our ECVs compared to ECVs performed in the context of RCTs could be explained by patient selection, variation in operator experience or technique, or variation in anesthetic management. Future studies should further evaluate the risk of NA for ECV in true practice scenarios outside of RCTs.
Repeat ECV with spinal anesthesia after a failed first attempt without spinal anesthesia increased vertex presentation at birth and decreased the rate of cesarean delivery.
Results: A total of 240 subjects were enrolled, and 239 received the intervention. External cephalic version was successful in 123 (51.5%) of 239 patients. Compared with bupivacaine 2.5 mg, the odds (99% CI) for a successful version were 1.0 (0.4 to 2.6), 1.0 (0.4 to 2.7), and 0.9 (0.4 to 2.4) for bupivacaine 5.0, 7.5, and 10.0 mg, respectively (P = 0.99). There were no differences in the cesarean delivery rate (P = 0.76) or indication for cesarean delivery (P = 0.82). Time to discharge was increased 60 min (16 to 116 min) with bupivacaine 7.5 mg or higher as compared with 2.5 mg (P = 0.004).
Conclusions: A dose of intrathecal bupivacaine greater than 2.5 mg does not lead to an additional increase in external cephalic procedural success or a reduction in cesarean delivery.
Trends are evolving in decreasing intraoperative and postoperative opioid use. Therefore, anesthesiologists are constantly learning new regional techniques to help with postoperative pain. For shoulder surgeries, I’ve moved away from interscalene blocks toward supraclavicular blocks. I think the interscalene block provides a better block of a total shoulder surgery, however, certain patient comorbidities often make the supraclavicular block a better choice.
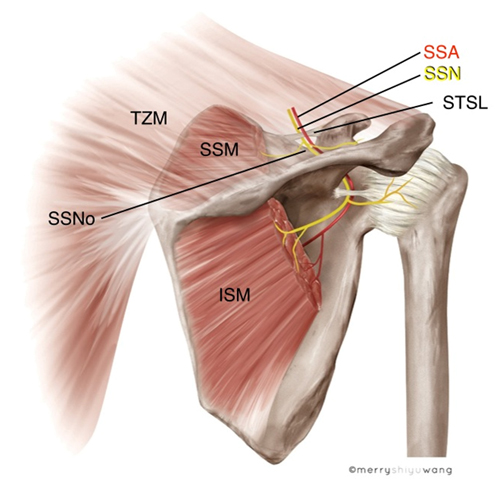
Conclusions: The anterior suprascapular block, but not the supraclavicular, provides noninferior analgesia compared to the interscalene approach for major arthroscopic shoulder surgery. Pulmonary function is best preserved with the anterior suprascapular nerve block.
Trends are evolving in decreasing intraoperative and postoperative opioid use. Therefore, anesthesiologists are constantly learning new regional techniques to help with postoperative pain. For shoulder surgeries, I’ve moved away from interscalene blocks toward supraclavicular blocks. I think the interscalene block provides a better block of a total shoulder surgery, however, certain patient comorbidities often make the supraclavicular block a better choice.
I’d love to incorporate my findings and use of lidocaine infusions and ketamine infusions on intraoperative and postoperative pain as a multimodal pain management pathway.
I’d love to incorporate my findings and use of lidocaine infusions and ketamine infusions on intraoperative and postoperative pain as a multimodal pain management pathway.